
Morgenstern, J. The 2022 American College of Cardiology guideline on the evaluation and disposition of acute chest pain, First10EM, October 26, 2022. Available at:
https://doi.org/10.51684/FIRS.128865
As part of the Rapid Review series, I try to highlight key points from important guidelines. I am not sure that this guideline from the American College of Cardiology rises to that level, but I had to review it to update the EM:RAP CorePendium chapter, so I might as well share a few take-aways. There is really only one recommendation that you must know: they acknowledge multiple STEMI-equivalents that should be treated in the same manner as traditional STEMI patients. However, there are a few other points worth raising.
The paper
Writing Committee, Kontos MC, de Lemos JA, Deitelzweig SB, Diercks DB, Gore MO, Hess EP, McCarthy CP, McCord JK, Musey PI Jr, Villines TC, Wright LJ. 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2022 Oct 6:S0735-1097(22)06618-9. doi: 10.1016/j.jacc.2022.08.750. Epub ahead of print. PMID: 36241466
Summary
Their assumptions about CCTA seem unfounded
I really like that they start out by explicitly stating their clinical assumptions. However, one of those assumptions sort of undermines the credibility of the paper. They state that “coronary computed tomography angiography (CTA) is an important tool for evaluation of intermediate-risk patients in the ED, and thus, broader application across centers and greater availability within centers is recommended.” That is an amazingly bold statement to be placed in the assumptions section of a paper. That kind of statement seems like it should be based on research, rather than an assumption, especially when the bulk of the research seems to suggest either no benefit or harm. For example, a systematic review of emergency department RCTs found no benefit in terms of death, MI, or MACE, but clear harm in an increase in invasive procedures. (Gongora 2018)
Later in the document, they state “The use of coronary CTA in patients presenting with acute chest pain is supported by numerous randomized clinical trials that enrolled predominately non–high-risk patients without previously known CAD.” However, the only citation they provide for this claim leads to this letter to the editor. For a huge peer reviewed publication, that is pretty bad. So again, I had already lost a lot of confidence in this guideline before I had even made it through the introduction. (Although, actually, most of the rest of the document is pretty reasonable.)
I like their assumption about clinical judgment (but it might be equally unfounded)
Also in the assumptions section, they state that “CDPs [clinical decision pathways] for rapid evaluation of chest pain should be interpreted within the context of all available clinical information. The provider’s clinical judgment at the bedside remains an indispensable tool that may lead to different triage decisions than those suggested by the CDP.”
In other words, you still need to be a doctor. You can over-rule these decision pathways. I think this is clearly correct, but I am not aware of any research that proves the fact, and as it is in their assumption section, they also don’t provide any citations.
Low risk patients don’t need more testing
They state that “patients classified as low risk (rule out) using hs-cTn–based CDPs supported by this document can generally be discharged directly from the ED without additional testing, although outpatient testing may be considered in selected cases.”
This is basically a re-iteration of the 2021 AHA guidelines, but we are now getting a very consistent message: low risk patients don’t need more testing. We already knew this, as the tests we generally order (stress tests or CCTA) are awful tests. We already knew we shouldn’t be ordering these tests. But many doctors have a hard time following evidence-based medicine. You now have multiple guidelines telling you to stop, so please stop.
Phasing out “atypical”
They support the suggestion made by the AHA to use the terms “cardiac”, “possible cardiac”, and “noncardiac” as replacements of “typical” and “atypical” chest pain. I still think this is a silly recommendation, as I wrote about in my summary of the AHA guidelines.
Moving beyond “STEMI”
I think the ECG section is the most important part of this document, and probably the only section that could change practice for most of us (as outside of America, almost all of us have been using these high sensitivity troponin pathways for years).
The big thing, in my mind, is that unlike the AHA they specifically name “STEMI equivalents”. That is a huge help, as the emergency community has known for quite some time that many acute coronary occlusions do not fit classic STEMI patterns.
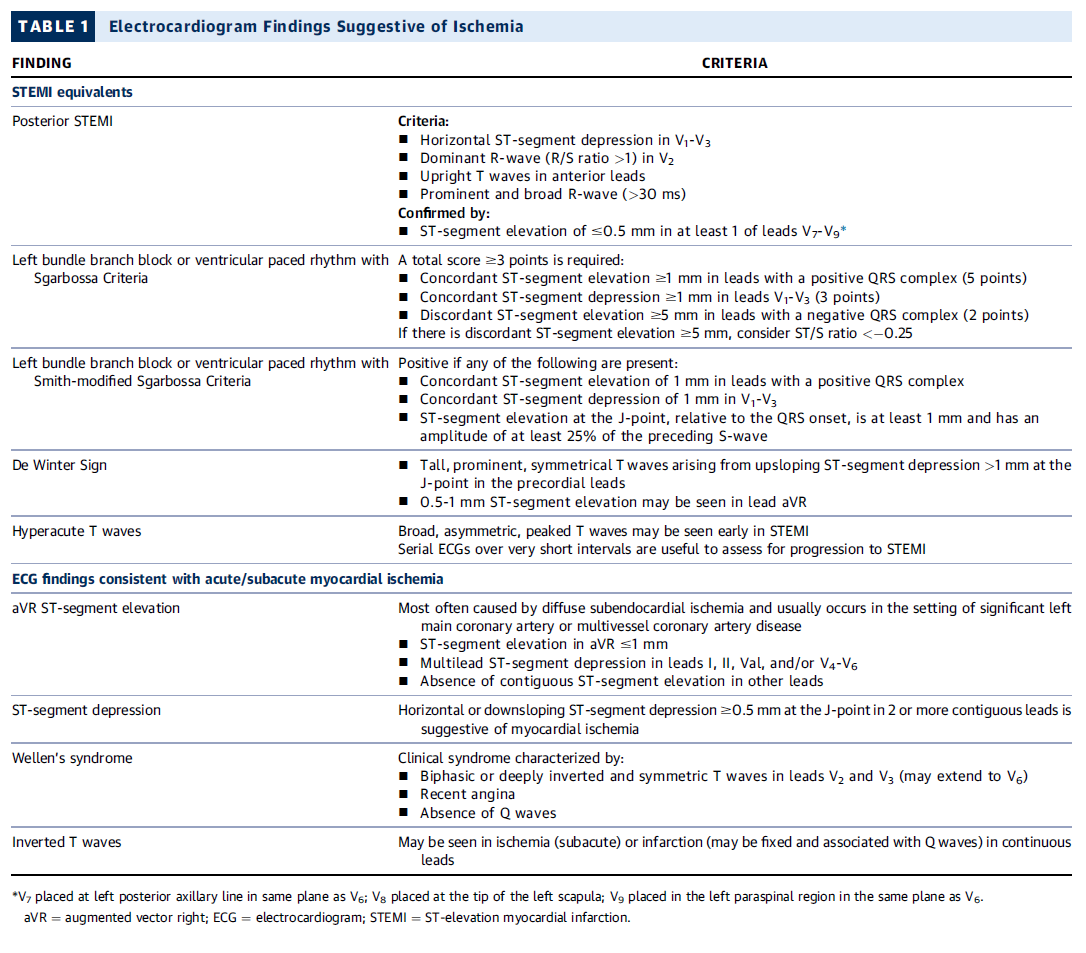
They state “in the absence of ischemic ST-segment elevation, the ECG should be examined for other changes that have been associated with coronary artery occlusion (see Table 1); when present, these should prompt evaluation for emergent coronary angiography.”
The ECG changes they count as STEMI equivalents are: posterior STEMI, Sgarbossa criteria in both LBBB and paced rhythm, De Winter sign, and hyperacute T waves. If you need examples of these ECG patterns, I would suggest Dr. Smith’s ECG blog or the ECG Cases blog as part of Emergency Medicine Cases.
They specifically endorse the Smith-modified Sgarbossa criteria, which is considered positive if there is “ST-segment elevation at the J-point, relative to the QRS onset, is at least 1 mm and has an amplitude of at least 25% of the preceding S-wave”, as it increases the sensitivity of the rule dramatically.
There are two other ECG findings that are also mentioned. They say Wellen’s syndrome should be managed as an NSTEMI. They specifically say “Wellen’s syndrome is characterized by biphasic or inverted T-wave inversions in the anterior precordial leads in patients whose ischemia has resolved. Its presence is associated with proximal left anterior descending artery stenosis and is associated with high rate of subsequent transmural MI.” I think this is probably a reasonable recommendation, but it highlights a major problem with our current terminology. NSTEMI covers way too broad a swath of patients. Most patients with small troponin bumps and normal ECGs actually have quite low risk. The value of cath in these patients is questionable. But a patient with Wellen’s is much higher risk than the average patient I admit with NSTEMI, and definitely needs a cath. Although the cath may not have to happen at 3am, there is no reason to delay it, so just saying “manage as per NSTEMI guidelines” might be too passive.
The final pattern they discuss is ST elevation in aVR with mutilead ST depression. If you just look at the figures, they also say this should be managed as NSTEMI, but the figures clash with their text, and I think the text is very important. They state that this pattern “represents a high-risk ECG finding that is associated with high morbidity and mortality. In patients with ischemic symptoms, this often represents diffuse ischemia due to significant stenosis involving the left main and/or 3-vessel disease, although it can be seen in other non-ACS conditions causing a demand/supply mismatch. In approximately 10% of cases, acute coronary occlusion is present. Accordingly, management of patients with this ECG pattern must be nuanced. Precipitants of supply/demand mismatch (if present) should be treated. Emergent coronary angiography should be considered in patients with persistent ischemic symptoms or ECG changes after treatment or if there is hemodynamic instability.” In my mind, the emphasis should be on the final part. Considering the high risk of acute coronary occlusion, it should be assumed that this ECG pattern requires emergent coronary angiography. Of course, we should ensure that the story fits, and there aren’t other causes of a potential supply/demand mismatch, but we should be doing that in all patients presenting with possible occlusion MI.
I think their comments about echocardiography, although probably true, are problematic for many emergency doctors
They state that “emergent transthoracic echocardiography (TTE) for assessment of wall motion should be considered in patients with ECGs concerning for but not diagnostic of ischemia and infarction, particularly when borderline ST-segment elevation or left bundle branch block (LBBB) or equivocal signs of posterior MI are present. Because accurate assessment of wall motion is difficult, the TTE should be performed and reviewed by a clinician qualified in echocardiography.”
From what I understand from my ultrasound focused colleagues, wall motion abnormalities can help a lot. I even try to look for them myself, but acknowledge I have neither the skill nor training to use the test with definitive accuracy. My concern is the phrasing, and the impact that guidelines have on medico-legal culture. The suggestion might be completely reasonable in theory, but for what percentage of emergency departments is this a realistic suggestion? How many places can get a formal echo 24/7? I certainly have never worked in such a place.
My concern is really just with the way guidelines are used, rather than the actual content of this recommendation. Guidelines are frequently (and inappropriately) used to define standard of care. Although they shouldn’t be used this way, I think guideline writers need to acknowledge that they are. Writers have a responsibility to be careful in the phrasing of the recommendations, knowing how their guidelines will ultimately be used. I think this statement should have been qualified to acknowledge that this is not the reality in the vast majority of emergency departments worldwide.
Detectable troponin is never normal, but it isn’t all ACS
We still need to be doctors. MI is not diagnosed based on troponin. It is diagnosed based on the history and physical, combined with our tests. At the end of the day, clinical judgment is an essential part of the diagnosis. However, even if an elevated troponin doesn’t indicated acute coronary syndrome, it is associated with bad outcomes.
They say “minor hs-cTn elevations are also associated with worse outcomes in ED patients who are ruled out for MI. Based on these findings, no detectable cTn level can be considered entirely “normal.” The higher the cTn value, the more likely it is related to ACS, although there is significant overlap among cTn values for type 1 and 2 MI and acute myocardial injury. As a result, hs-cTn values still require interpretation based on the appropriate clinical context.”
We should be using age and sex adjusted troponin thresholds
Personally, I have never worked in a hospital that does this, but it was suggested in the 2021 AHA guideline and is reiterated here.
“Troponin levels are higher in men than in women and increase with age in both sexes, even after excluding individuals with subclinical structural heart disease using a combination of ECGs, imaging tests, and established biomarkers.”
“Use of uniform 99th percentile URLs results in decreased sensitivity and negative predictive value (NPV) in women, contributing to the existing sex bias in the diagnosis and treatment of women with possible ACS. Use of sex-specific cutoffs can decrease the problem of MI underdiagnosis in women.”
MI can be ruled out with a single high sensitivity troponin at time zero in many patients
“Immediate disposition of approximately 25% to 50% of chest pain patients is possible in those who have a single undetectable or very low hs-cTn value, provided symptoms started >3 hours before the hs-cTn measurement (“0-hour rule out”).”
Clinical decision pathways using either 0 and 1 hour or 0 and 2 hour high sensitivity troponins are recommended
In one of the most pointless things I have ever seen said in a guideline, the state that “for inclusion in a CDP, we recommend that the patient have a nonischemic 12-lead ECG.” They feel like they need to state this because not all studies have explicitly stated it, but think about what they are actually saying. They are saying that in order to use a pathway designed to exclude ischemia, you shouldn’t include patients with objective evidence of ischemia. I probably could have left this out, because I think my readers are smart enough to sort that out.
“The ESC 0/1 (or 0/2) and High-STEACS approaches are recommended over simply using the 99th percentile URL value at 0 and 3 hours to rule out MI because direct comparisons demonstrate both greater efficacy (more patients ruled out) and greater safety (fewer missed MIs). Thus, hs-cTn should be implemented in the context of a CDP to achieve maximal performance.”
They do call out Americans for over-testing. They tell us that when these pathways were studied in Europe, they had positive predictive values of approximately 75% for the high risk group. However, because these pathways are applied to a much broader and lower risk population, in American studies the positive predictive value is much lower (from 20-50%). Therefore, “given the low PPV for MI when these CDPs are used broadly (as is typical for U.S. EDs), we recommend avoiding the term rule in for these algorithms and instead classifying this group as “abnormal.” Personally, I think that is the wrong recommendation. The correct recommendation is to only apply pathways designed for ACS to patients who actually have some risk for ACS.
Risk scores don’t help
Personally, I do not use the HEART score. Doing so would result in harm in my population, with a significant increase in unnecessary hospital admissions. ECG and troponins alone are more than enough in the vast majority of patients. These guidelines agree.
They say: “The 2021 AHA/ACC/multisociety chest pain guideline advises that patients who are ruled out by an hs-cTn CDP and have a nonischemic initial ECG may be discharged without further testing and do not require the application of risk scores. Indeed, randomized clinical trials that demonstrated safety and efficacy of the ESC 0/1-hour algorithm, the HIGH-STEACS algorithm, and single baseline hs-cTn rule-out pathways did not mandate the use of risk scores to identify patients at low risk.”
“Among 1,935 patients with suspected ACS, Chapman et al found that the addition of risk scores did not further improve the safety of the ESC 0/1-hour and High-STEACS pathways but decreased the number of patients identified as low risk.”
“Although routine application of risk scores for patients identified as low risk by these pathways is not recommended, the modified HEART score or EDACS may be considered for selective application especially in cases where the physician believes the patient may be higher risk based on their clinical history or symptoms at presentation.”
The treatment is different, but don’t downplay the importance of type 2 MI
“CAD is common among patients with type 2 MI when imaging is systematically applied; approximately two-thirds have CAD and one third have obstructive disease. Furthermore, one third have left ventricular dysfunction detected on imaging. Following discharge, major adverse cardiovascular events are higher when compared with type 1 MI due to a greater comorbidity burden and risk of noncardiovascular mortality.”
“If there is uncertainty regarding whether the diagnosis is a type 1 or 2 MI, clinicians should generally manage the patient as presumed type 1 MI.”
Seriously, stop with the stress tests
Not only are they bad tests, they are probably testing the wrong organ system. Few patients who are ruled-out with normal ECGs and multiple high sensitivity troponins will have a cardiac cause of their chest pain. Sending them for cardiac testing is not only harmful because of the massive number of false positives, but also because you are likely delaying diagnosis of whatever the real problem is.
“Patients ruled out using an hs-cTn CDP are eligible for discharge from the ED without further noninvasive cardiac testing due to their low likelihood of 30-day death and MI.”
“Given that most patients will have a noncardiac etiology for their chest pain, evaluation for alternative, non–ACS-related cardiac and noncardiac conditions should be performed as clinically appropriate.”
Of course, close follow up is important, but it is almost certainly better to see your family doctor than a cardiologist.
References
Gongora CA et al. Acute Chest Pain Evaluation using Coronary computed tomography Angiography Compared with Standard of Care: A Meta-Analysis of Randomised Clinical Trials. HEART 2018. PMID: 28855273
Writing Committee, Kontos MC, de Lemos JA, Deitelzweig SB, Diercks DB, Gore MO, Hess EP, McCarthy CP, McCord JK, Musey PI Jr, Villines TC, Wright LJ. 2022 ACC Expert Consensus Decision Pathway on the Evaluation and Disposition of Acute Chest Pain in the Emergency Department: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2022 Oct 6:S0735-1097(22)06618-9. doi: 10.1016/j.jacc.2022.08.750. Epub ahead of print. PMID: 36241466


2 thoughts on “The 2022 American College of Cardiology guideline on the evaluation and disposition of acute chest pain”