Morgenstern, J. More evidence against hypothermia (HACA-IHCA), First10EM, October 3, 2022. Available at:
https://doi.org/10.51684/FIRS.128583
I have covered post-arrest hypothermia at length on this blog. (For example, here, here and here.) Although we are still waiting for definitive answers, I have always been rather skeptical, and the more trials we see, the more certain it is becoming that this whole enterprise was just a waste of everyone’s time and money. There is a new RCT (HACA-IHCA) to look at. It won’t convert any hypothermia true believers, and will probably bore those who already don’t believe, so I will try to keep my summary short. The big difference is that this trial looks at in-hospital cardiac arrest, which generally means faster response times, better outcomes, and therefore the best possible conditions for hypothermia to succeed.
The paper
HACA-IHCA: Wolfrum S, Roedl K, Hanebutte A, Pfeifer R, Kurowski V, Riessen R, Daubmann A, Braune S, Söffker G, Bibiza-Freiwald E, Wegscheider K, Schunkert H, Thiele H, Kluge S. Temperature Control After In-Hospital Cardiac Arrest: A Randomized Clinical Trial. Circulation. 2022 Sep 28:101161CIRCULATIONAHA122060106. doi: 10.1161/CIRCULATIONAHA.122.060106. PMID: 36168956 [free full text]
The Methods
“The HACA-IHCA (Hypothermia After IHCA) trial was an investigator-initiated, multicenter, open-label, blinded outcome–assessed, randomized, controlled trial.”
Patients
Adult patients who remained unconscious (GCS <9) more than 45 minutes after inpatient cardiac arrest. Patients were eligible irrespective of cardiac rhythm or etiology of arrest.
Intervention
Temperature control with a target between 32 and 34 degrees Celsius for 24 hours, followed by slow rewarming.
Comparison
Temperature control with a target of normothermia. (No specific protocol was followed, it was just strongly recommended to avoid temperatures greater than 37.5 Celsius).
Outcome
The primary outcome was all cause mortality at 180 days.
The Results
Of 1055 patients assessed for eligibility, 249 were randomized, and 238 are included in the final analysis. (Their sample size calculation called for 440 patients).
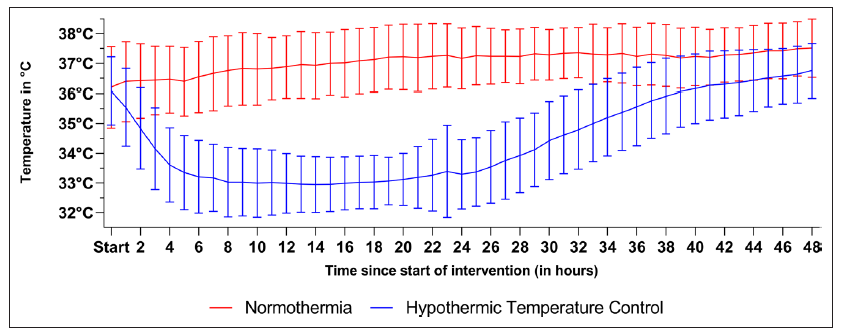
They failed to hit their target temperature in the hypothermia group in 28% of patients. The mean temperature at 12 hours was 34.0 degrees. I don’t think they report how many patients in either group became febrile, but unlike some of the other trials, the plotted temperatures all seem to stay below 38 degrees.
The groups weren’t perfectly balanced, with the normothermia group having slightly more patients with shockable rhythms.
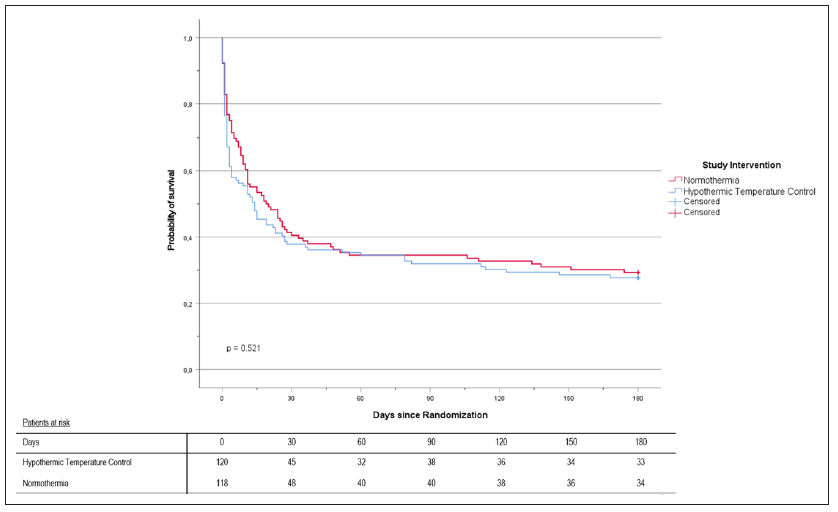
There was no difference in the primary outcome of mortality. It was 72.5% with hypothermia and 71.2% with normothermia, RR 1.03, 95% CI 0.79-1.40, p=0.89.
There was also no difference in neurologic outcomes, with a favourable outcome being seen in approximately 82% of the survivors in both groups.
My thoughts
There are many problems with this RCT. They missed their target temperature in the treatment group more than a quarter of the time, and the treatment group may have had worse prognostic features at the outset.
The decision to withdraw life support was not protocolized, but rather left to the treating physicians. Patients were enrolled between 2007 and 2014, and these decisions were often made using different criteria than we use a decade later.
Blinding will always be an issue with hypothermia trials. The care team, patient, and families could not be blinded, as body temperature is pretty apparent to anyone coming into contact with the patient. For the fairly objective primary outcome of all cause mortality, the lack of blinding shouldn’t matter much, but it does make neurologic outcomes hard to judge in all these trials.
The trial was stopped early for futility, but there was no predetermined criteria for this decision. The end result is a study less than half the size that they calculated was required to identify a 16% absolute decrease in all cause mortality. In itself, designing a trial with the thought you might see a 16% decrease in mortality is ridiculous. That is an unheard of difference, so you are just setting the trial up for failure from the beginning. (People often just play with sample size calculations to justify the number of patients they think they can enroll, rather than truly designing a study that will answer an important scientific question. That wasn’t what happened here. Instead they used the unbelievable results of the original HACA trial to guide their sample size calculation.) If these authors had been more reasonable when designing the study, they probably would have designed a trial at least 10 times this big, so we are left with a dataset that is extremely under-powered.
This trial took a surprisingly long time to be published. The last patient was enrolled in May of 2014. That was 8 years ago! Even with the 180 days of follow-up data that was required, it seems crazy that it took this long to get published. I don’t know who to blame, but this is indicative of a massive problem with our current scientific structures, especially when you compare it to the press-release ‘science’ that has occurred during the pandemic when companies stood to make money.
Despite the shortcomings, I do think HACA-IHCA is an important addition to our hypothermia dataset. Outcomes are much better after inpatient cardiac arrest (more than 25% of both of these groups were alive half a year later). One of the biggest concerns in out of hospital cardiac arrest research is that outcomes are so bad in both groups, even effective treatments could be overlooked because we are attempting to apply them to patients who are already totally (not reversibly) dead.
Bottom line
HACA-IHCA is too small and too flawed to add much to the overall debate, but it is another small piece of data that suggests hypothermia is not needed after cardiac arrest.
Other FOAMed
Hypothermia for cardiac arrest
TTM2: The big chill on ‘therapeutic’ hypothermia
Journal Jam 19 Therapeutic Hypothermia After Cardiac Arrest – Mixed Evidence
PulmCrit – A history of hypothermia for cardiac arrest, 2002-2021 (RIP)
References
Wolfrum S, Roedl K, Hanebutte A, Pfeifer R, Kurowski V, Riessen R, Daubmann A, Braune S, Söffker G, Bibiza-Freiwald E, Wegscheider K, Schunkert H, Thiele H, Kluge S. Temperature Control After In-Hospital Cardiac Arrest: A Randomized Clinical Trial. Circulation. 2022 Sep 28:101161CIRCULATIONAHA122060106. doi: 10.1161/CIRCULATIONAHA.122.060106. PMID: 36168956 [free full text]

One thought on “More evidence against hypothermia (HACA-IHCA)”