Despite ‘therapeutic’ hypothermia’s widespread use, the evidence for the practice has always been weak. I went through that evidence here. At that point, I tried to be optimistic, given the potentially positive results of the HYPERION trial, but I also noted the many problems with HYPERION that left me skeptical. (Lascarrou 2019) We now have the TTM2 (targeted temperature management 2) trial, which pretty clearly demonstrates that there is nothing therapeutic about ‘therapeutic’ hypothermia.
The paper
Dankiewicz J, Cronberg T, Lilja G, et al: TTM2 Trial Investigators. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. N Engl J Med. 2021 Jun 17;384(24):2283-2294. doi: 10.1056/NEJMoa2100591. PMID: 34133859 NCT02908308
The Methods
TTM2 is an international, multi-center, randomized trial.
Patients
Comatose adult patients admitted to hospital after an out of hospital cardiac arrest, irrespective of initial rhythm. Patients had to have at least 20 minutes of ROSC before being enrolled, but were excluded if more than 180 minutes had passed, or it was an unwitnessed arrest with asystole as the presenting rhythm.
Intervention
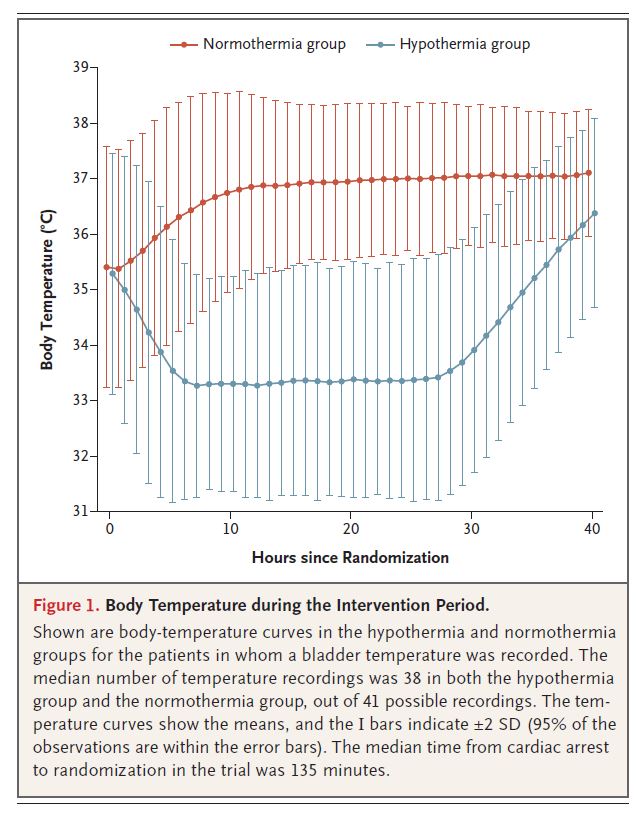
Hypothermia: A target temperature of 33 degrees Celsius, maintained for 28 hours, and then slowly rewarmed by 1 degree every 3 hours.
Comparison
Normothermia: Aim to maintain a temperature of 37.5 degrees Celsius or less.
Outcome
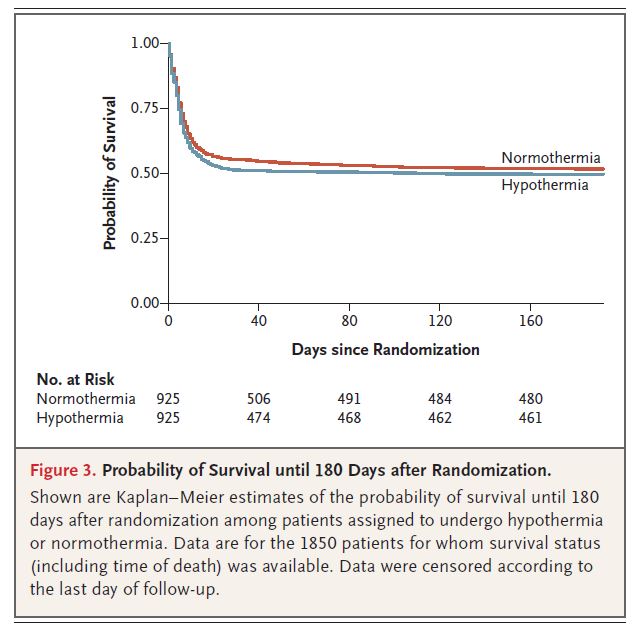
The primary outcome was death from any cause at 6 months.
The Results
They included 1861 patients. The mean age was about 64, and 80% were male. About 75% had a shockable rhythm. 90% had a witnessed arrest, and 80% received bystander CPR. It took a mean of 3 hours to reach the target temperature in the hypothermia group.
Hypothermia didn’t work. There was no difference in all cause mortality (48% versus 50%, p= 0.37). There was no difference in functional outcomes or quality of life. The lack of benefit was consistent across all subgroups.
Arrhythmias were more common in the hypothermia group (24% versus 16%, p<0.001). The hypothermia group also needed more paralytics, and ended up on mechanical ventilation for longer.

My thoughts
This is an excellent trial, and combined with the original TTM trial, represents a higher level of evidence than the original hypothermia RCTs. That being said, no trial is perfect. The biggest problem with this trial is that it didn’t include a no treatment group. Ever since the first TTM trial, people have been arguing that fever control is absolutely essential. However, as one of this paper’s authors points out, there is no good evidence that maintaining normothermia (ie preventing fever) helps. Fever control has not actually been studied in this population, but when looking at all ICU patients, there are RCTs that show pretty clearly that fever control does not help. (Young 2019) (Yes, there is observational data showing that fever is associated with worse outcomes, but that doesn’t mean that controlling fever will improve outcomes. There is a strong association between ice cream sales and drownings in public pools, but that doesn’t mean that banning ice cream will somehow prevent drownings.) The design of this trial means that there will still be a strong contingent arguing, without any strong evidence, that we must avoid fever at all costs. Personally, I think the burden of proof lies firmly in their court at this point, and we should stop the costly practice of temperature control until there is actually evidence it helps.
Although it turned out not to matter in this trial, because there were no differences in any outcomes, all cause mortality is probably not as good a primary outcome as survival with good function (although it is far more objective). From a critical appraisal standpoint, I think it is important to remember that mortality in a modern ICU is not nearly as objective as it sounds. We have a lot of control over when people die, and that can matter a lot in an unblinded trial. However, to get around that subjectivity, this trial had blinded clinicians perform standardized exams at 96 hours for neuroprognostication. It’s not perfect, as the primary team was unblinded and was responsible for clinical decisions, but it is an important step to reducing bias.
Hypothermia is one of those therapies that has very strong supporters. We are likely to hear a lot about flaws with this study. That is not a problem – critical appraisal is always welcomed. However, my guess is that the much bigger flaws in the original hypothermia RCTs will simultaneously be downplayed, and that is a problem. At this point, the TTM and TTM2 trials are clearly the biggest and highest quality studies we have, and the results are pretty clear: there is no ‘therapeutic’ in hypothermia. In fact, due to the increase in adverse events, hypothermia appears to be net harmful.
Whether there is any benefit from fever prevention, or temperature management of any sort, remains to be seen. I think the burden of proof now clearly lies with those arguing in favour of the practice. We don’t need observational data. We need RCTs showing benefit. Until we see RCTs demonstrating benefit from temperature control, it is time to ditch the practice.
Hypothermia and the TTM2 trial stand as a great reminder of the mistakes that we make time and time again in medicine. We fall prey to the intervention bias. (Foy 2013) We are overly optimistic about small studies that are nowhere close to scientifically definitive, and quickly crown borderline practices as ‘silver bullets’ or ‘standard of care’. Think thrombolytics for stroke. Think TXA for just about anything (the topic of next week’s post). Think cardiac stress testing. Science is a process that requires replication. Single studies never define truth.
This overzealous adoption of medical practices hurts our patients. Time and time again, we adopt medical interventions that are unproven. In many cases, the harms end up outweighing the benefits, but we only acknowledge this decades later, when replication studies are finally done. We then act shocked about this ‘medical reversal’ that EBM experts were predicting all along. We spend tremendous amounts of money completely overhauling medical systems, ignoring the tremendous scientific uncertainty that remains. We balk at the time and effort required to complete confirmatory RCTs, but completely ignore the much larger expenditure we make adopting (and then de-apoting) unproven practices.
This overzealous adoption of medical practices also hurts evidence based medicine. EBM experts who point out the uncertainty are labelled as nihilists. When every Cochrane review concludes “more studies are needed”, people downplay the importance of science in medicine. They argue that we would never do anything if we waited on science. But the problem is, more studies are needed (especially in medicine, where we have adopted the laughable standard of p=0.05).
In emergency medicine, we are very good at handling clinical uncertainty. It doesn’t paralyze us. It doesn’t mean that we don’t act. We just acknowledge that our actions are provisional. We know that bad mistakes occur when we act overly certain. For some reason, we are much less comfortable accepting that same uncertainty when it exists in science.
From the day that the original hypothermia papers were published, the EBM community highlighted the remaining uncertainty. It was clear that more trials were needed, and many anticipated that those trials would be negative. Acknowledging uncertainty is not the same as proclaiming ineffectiveness. In the face of uncertainty, we need to judge the potential benefits, known harms, and degree of uncertainty, to determine our provisional action. Frequently, that means adopting a therapy while waiting on further trials. The problem is not using a treatment with imperfect evidence. The problem is ignoring the fact that the evidence is imperfect, and declaring an intervention the ‘standard of care.’ That is a mistake we make time and again in medicine.
Unfortunately, I doubt this trial is going to change many minds. Despite the clearly negative results, an accompanying editorial concludes that “targeted temperature management… is a crucial treatment strategy to improve outcomes in patients who have had a cardiac arrest.” (Morrison 2021) Considering the evidence we have available, I really don’t understand that conclusion. There is definitely still uncertainty. Targeted temperature management could have a role, but the best available evidence runs counter to that hypothesis. There was probably never anything therapeutic about ‘therapeutic’ hypothermia.
Bottom line
This large RCT demonstrated no benefit from ‘therapeutic’ hypothermia as compared to managed normothermia. To date, there is no evidence that managed normothermia is any better than no temperature management at all. That study probably needs to be done, but until then, temperature should not be a priority in post-arrest care.
Other FOAMed
PulmCrit – A history of hypothermia for cardiac arrest, 2002-2021 (RIP)
References
Dankiewicz J, Cronberg T, Lilja G, et al: TTM2 Trial Investigators. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. N Engl J Med. 2021 Jun 17;384(24):2283-2294. doi: 10.1056/NEJMoa2100591. PMID: 34133859
Foy AJ, Filippone EJ. The case for intervention bias in the practice of medicine. Yale J Biol Med. 2013 Jun 13;86(2):271-80. PMID: 23766747
Lascarrou JB, Merdji H, Le Gouge A, et al. Targeted Temperature Management for Cardiac Arrest with Nonshockable Rhythm. The New England journal of medicine. 2019; 381(24):2327-2337. PMID: 31577396 [full text] NCT01994772
Morrison LJ, Thoma B. Translating Targeted Temperature Management Trials into Postarrest Care. N Engl J Med. 2021 Jun 17;384(24):2344-2345. doi: 10.1056/NEJMe2106969. PMID: 34133865
Young PJ, Bellomo R, Bernard GR, et al. Fever control in critically ill adults. An individual patient data meta-analysis of randomised controlled trials. Intensive care medicine. 2019; 45(4):468-476. PMID: 30741326
Morgenstern, J. TTM2: The big chill on ‘therapeutic’ hypothermia, First10EM, June 21, 2021. Available at:
https://doi.org/10.51684/FIRS.80469


8 thoughts on “TTM2: The big chill on ‘therapeutic’ hypothermia”
I’m just gonna leave these quotes here to emphasize your points in the discussion – hopefully more and more pressure can be put on the system to change the culture of research- and science in medicine. Thanks for another great post!
“I think there is both overuse and underuse in healthcare …in most developed countries … we’re spending so much and wasting so much that “healthcare” is one of the leading public dangers for health . It’s possible that our society will disintegrate just because we’re wasting too much or trying to do too much that has very little evidence or even has evidence that it is unnecessary . It’s a major threat and something that everyone interested in health needs to fight against. I think at some point we need to fight against medicine – it’s becoming really dangerous
There are … conflicts from physicians / everyone involved in healthcare . It can be really hard to disentangle from the fact that we are specialists (that we have some reason of existence ) and our reasons of existence may be related to doing some particular procedures or doing some type of medicine that may be threatened by evidence . How likely is it that we will design studies that will show that what we do is something that needs to be abandoned, that we need to change jobs , that we are not relevant , not needed in order for people to have better health . I think that adds another layer of conflict that is very difficult to disentangle”
John Ioannidis, The recommended dose podcast (https://m.soundcloud.com/therecodo/09-john-ioannidis )
“It is difficult to get a man to understand something when his salary depends upon his not understanding it”
Upton Sinclair (often quoted in this context by Jerome Hoffman)
“One of the lessons of medical reversal is that horses are very difficult to rein in once they are loose
No one can decide what new medical technology to adopt simply based on how it looks. If you cannot judge a book by its cover, you certainly cannot judge a medical innovation by its promise ”
Cifu and Prasad: Medical Reversal
He [Schopfenhauer] maintained that all truth passes through three stages: first, it is ridiculed; second, it is violently opposed; and finally, it is accepted as having always been self evident
Bernard Lown, The Lost Art of Healing
Thanks!
I could have skipped the writing and just used the quotes instead 🙂
No no! Apparently it’s worth repeating and continue to highlight examples , as you’ve done brilliantly . This cruise ship takes some time to turn around
“From a critical appraisal standpoint, I think it is important to remember that morality in a modern ICU is not nearly as objective as it sounds.”
Uhm… while that may be true, I do think you meant “morTality”
Haha
Not the first time I have made this type – and it always seems to add multiple layers of hidden meaning
Thanks for catching it