
Morgenstern, J. The PEACH trial of seizure prophylaxis for head bleeds: Not such a peach, First10EM, October 10, 2022. Available at:
https://doi.org/10.51684/FIRS.128649
I first heard about this article on Scott Weingart’s RACC Lit review, where he discussed it as a practice changing paper. In that context, I was excited to read it. I downloaded it as soon as I got out of the car. I will admit, I was pretty biased at the beginning, because Scott is right about almost everything, so I started my write up with a very positive slant. However, the more time I spend with this paper, the worse it seems. (We are talking about the PEACH trial, an RCT of prophylactic levetiracetam in spontaneous intracerebral hemorrhage.)
The paper
The PEACH trial: Peter-Derex L, Philippeau F, Garnier P, et al. Safety and efficacy of prophylactic levetiracetam for prevention of epileptic seizures in the acute phase of intracerebral haemorrhage (PEACH): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol. 2022 Sep;21(9):781-791. doi: 10.1016/S1474-4422(22)00235-6. PMID: 35963261 ClinicalTrials.gov NCT02631759
The Methods
The PEACH trial was a double-blind, randomized, placebo-controlled trial.
Patients
Adult patients with spontaneous supratentorial intracerebral hemorrhage (diagnosed on CT or MRI) presenting with 24 hours of symptom onset.
Exclusions: NIHSS scale greater than 25, bleeds thought to be secondary to trauma, vascular malformation, tumor, or ischemic stroke, current use of an antiepileptic, severe depression or psychotic disorder, known terminal illness, pregnancy, and the occurrence of a seizure between the time of enrollment and initiation of treatment.
Intervention
Levetiracetam 500 mg IV BID for 2 days, the 500 mg PO BID for 1 month, then a taper for 2 weeks. (Note: these are much lower doses than we are giving in status epilepticus.)
Comparison
Matching placebo.
Outcome
Any seizure within 72 hours of enrollment, whether clinically obvious, or just seen on EEG.
The Results
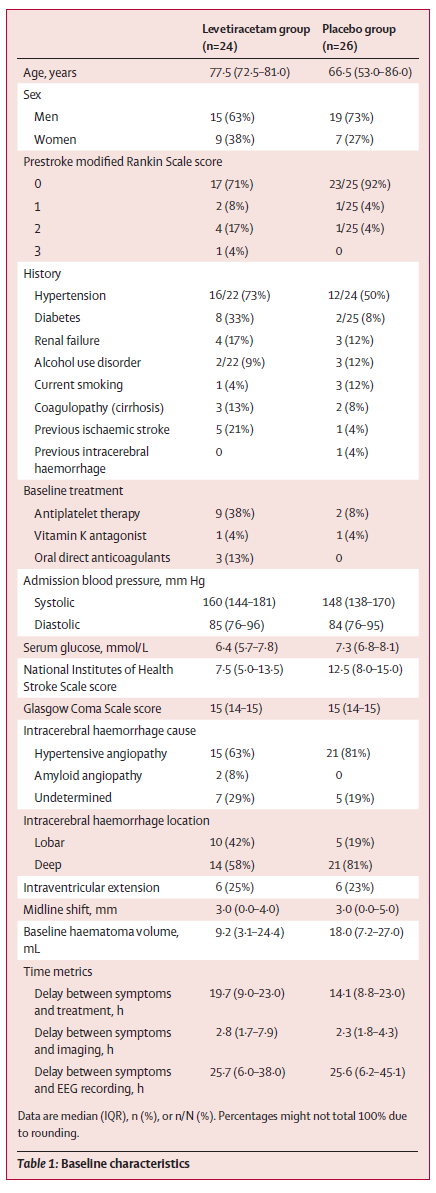
They enrolled 50 patients (of the 102 they were planning to enroll), and included 42 in their statistical analysis. There were significant baseline differences between the groups.
For the primary outcome of any seizure at 72 hours, there as a large and statistically significant difference between the groups, with 16% of the levetiracetam group and 43% of the placebo group having seizures (OR 0.16, 95% CI 0.03-0.94, p=0.043).
None of the clinical outcomes had statistically significant results, whether it was measured by change in NIHSS or mRS. Quality of life did not differ at 3,6, or 12 months.
My thoughts
Although this is a reasonable question, and an important trial to do, I think this is very clearly not a practice changing paper. (Sorry Scott).
The primary outcome of this trial is problematic. They were looking only at the occurrence of acute seizure, but they admit in their introduction that it is unclear whether acute seizures are important. Some studies have found an association with long term outcomes, but others have not. Acute seizure is being used as a surrogate outcome, but it is very unclear whether it is a surrogate of anything important. Additionally, they mix clinical seizures with seizures that are only identified by continuous EEG, which they tell us is not routinely done for intracerebral hemorrhage patients, and so may entirely represent over-diagnosis.
This is especially important, as there was not a single clinical seizure. I will say that again: there were 0 clinical seizures in both groups during the 72 hour timeframe. Over the 30 day treatment period, there was one clinical seizure in the placebo group and none in the treatment group, but this was obviously not statistically significant (p>0.99). The entire difference in this trial was based on continuous EEG monitoring. Considering that they tell us that outside of the trial they do not use continuous EEG monitoring, the entire difference this trial reports would have been completely invisible to them in the normal care of their patients. No one would have known. This is a tree falling in the woods situation, except we have decided to monitor very closely for that tree with advanced technology which we don’t know how to interpret.
They did follow these patients for 12 months, with a combination of in person visits and phone follow-ups. I have discussed before that the modified Rankin score is not reliable, especially when done by phone, which could skew results in either direction. However, there were no differences seen in any of the clinical or patient important outcomes. “The change in the NIHSS scores at 72 h, 1 month, or 3 months did not differ between groups, nor did the change in mRS scores at 3 months, 6 months, or 12 months.” Additionally, “quality of life assessed by the Stroke Impact Scale did not differ between groups at 3 months, 6 months, or 12 months.” So we are left only with a difference in a questionable surrogate outcome, without any difference in the long term clinical outcomes we all care about.
This study is way too small. Even as the study was designed, it was way too small. They based their power calculation on the assumption that they would see a 25% absolute benefit from treatment, which is an absurdly large number when prior trials of seizure prophylaxis have shown no benefit. Based on that calculation, they determined that they needed 102 patients enrolled, but they only ended up with 50 total, and the trial was stopped early without a predetermined stop point (because of slow enrollment, funding issues, and the COVID pandemic). On top of that, they exclude another 8 patients from their analysis for a variety of reasons, so the main analysis only has 42 patients. The result is a trial that is much too small to judge important outcomes.
Not surprisingly, because the trial is quite small, the groups look very dissimilar at baseline. The treatment group had more comorbidities, but the NIHSS score was higher in the placebo group and the hematoma size was twice as big in the placebo group. I would expect that worse strokes and larger hematomas would result in more seizures. (Seizures are harder to predict than other outcomes we see, so I don’t know which way I expect this trial to be biased, but I think the mismatch between the groups has a high chance of biasing the outcomes.)
Compliance was not great, but it was about the same in both groups. Only about 75% of patients took their medication without interruption for 1 month. This would likely bias against the treatment arm, although it probably represents real world usage, and therefore the effects we would see in clinical practice.
As I have discussed in the EBM bibliography, we see a disproportionate number of studies with p values just below the ‘significant’ threshold. With a p-value of 0.043, this trial fits into that general theme. That doesn’t mean anything in itself, as many trials will have legitimate p-values just below the threshold, but we know that as a whole, there are too many p-values reported at this level. Therefore, across all medicine, p-hacking must be occurring. I don’t know how to translate that information into a critical appraisal of a single paper, but we should always be skeptical of individual papers with borderline statistical results. This is one of the many reasons that replication of research is absolutely necessary before we assign any degree of certainty to the results.
Perhaps related to the theme of p-hacking, it is very concerning when published trials do not match their registered protocols, especially when there is no explanation. This trial is registered on clinicaltrials.gov, and it is very clear that they were measuring outcomes for 48 hours. That isn’t mentioned at all in the manuscript, where instead they report on 72 hour outcomes. Considering that they report that “the median period between intracerebral hemorrhage symptom onset and the first recorded electrographic seizure was 45·7 h [IQR 30·6–55·7] in the levetiracetam group and 49·8 h [32·4–53·9]”, it seems like at least half of the seizures occurred outside of their original study time frame, and it is very likely that if they had followed their study protocol, this would have been a negative trial.
Bottom line
I do not believe the PEACH trial should change practice. There is no change in clinical seizures and no change in clinical outcomes. Levetiracetam may decrease the number of seizures seen on continuous EEG monitoring (although I think this is a low certainty result given the size of the study, early stopping, and imbalance between the groups). However, EEG seizures are a surrogate outcome without clear association to clinical outcomes. Larger trials with a focus on clinical outcomes are required to drive clinical practice change.
Note: Scott has clarified with me that he was not passing judgement on whether this paper should change practice, just making the comment that, knowing the practice of neuro-ICUs, it will change practice, and we should be prepared to hear that recommendation from our specialists.
Other FOAMed
EMCrit RACC-Lit Review for September 2022
References
Peter-Derex L, Philippeau F, Garnier P, et al. Safety and efficacy of prophylactic levetiracetam for prevention of epileptic seizures in the acute phase of intracerebral haemorrhage (PEACH): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Neurol. 2022 Sep;21(9):781-791. doi: 10.1016/S1474-4422(22)00235-6. PMID: 35963261
Image by <a href=”https://pixabay.com/users/u11116-8530157/?utm_source=link-attribution&utm_medium=referral&utm_campaign=image&utm_content=3314679″>Margo Lipa</a> from <a href=”https://pixabay.com//?utm_source=link-attribution&utm_medium=referral&utm_campaign=image&utm_content=3314679″>Pixabay</a>
One thought on “The PEACH trial of seizure prophylaxis for head bleeds: Not such a peach”