In the Rapid Review series, I briefly review the key points of a clinical review paper (or two). The topic this time: Cerebral venous thrombosis (CVT)
The papers:
Behrouzi R, Punter M. Diagnosis and management of cerebral venous thrombosis. Clin Med (Lond). 2018;18(1):75-79. doi:10.7861/clinmedicine.18-1-75 PMID: 29436443
Long B, Koyfman A, Runyon MS. Cerebral Venous Thrombosis: A Challenging Neurologic Diagnosis. Emerg Med Clin North Am. 2017;35(4):869-878. doi:10.1016/j.emc.2017.07.004 PMID: 28987433
What is cerebral vein thrombosis?
The name sort of says it all. This is a thrombosis of the cerebral veins and/or major dural sinuses. (It is the DVT syndrome of the brain.) The symptoms and pathology arise from a combination of increased intracranial pressure, hemorrhage, and edema.
How common is it?
It has an incidence of about 1 case per 100,000 people per year. It makes up 0.5% of all stroke syndromes.
Who gets it?
Cerebral venous thrombosis tends to present in younger patients, with a mean age of 39 years, and 80% of patients presenting under the age of 50. It is 3 times more common in females than males, although that disparity disappears in older patients, in whom cancer is the primary risk factor.
Up to 90% of patients with cerebral vein thrombosis have at least one risk factor for venous thromboembolism. Thrombophilias are present in more than 30% of patients, but often aren’t diagnosed until after the CVT. Localized infections, such as osteomyelitis or mastoiditis can also provoke CVT.
How does it present?
Unfortunately, this is a very difficult diagnosis to make, in large part because it can present in so many different ways, depending on the extent and location of the thrombus, and whether there is associated hemorrhage, raised intracranial pressure, or mass effect. There are four major CVT syndromes: isolated intracranial hypertension (the most common), focal neurologic abnormality, seizure, and encephalopathy.
Headache is the most common presenting symptom. It is present in 90% of patients and is the only symptom in 25%. However, the description of the headache is highly variable, from localized pain, to a migraine like description, to a thunderclap headache similar to subarachnoid hemorrhage, to a positional headache related to raised intracranial pressure.
Focal neurologic deficits will be present in about 40% of patients. Seizures will also be present in about 40% of CVT patients. A smaller number of patients will present with full blown encephalitis, due to extensive hemorrhage, edema, and/or herniation.
The timing of presentation is also highly variable, with acute, subacute, and chronic presentations.
When do we need to think about this in the ED?
There will be a large variety of presentations, but I think it is essential to consider this diagnosis in a few key scenarios:
- An otherwise unexplained severe or prolonged headache in patients with thrombotic risk factors.
- Symptoms consistent with raised ICP or unexplained papilledema, especially in a younger patient with thrombotic risk factors.
- A thunderclap headache in a patient with thrombotic risk factors who rules out for subarachnoid hemorrhage.
- Stroke patients who present with seizure, severe headache, or neurologic findings that do not fit clear arterial distributions.
- Intracranial hemorrhage that doesn’t fit a classic pattern, especially if there are multiple bleeds, or the patient is young.
How is it diagnosed?
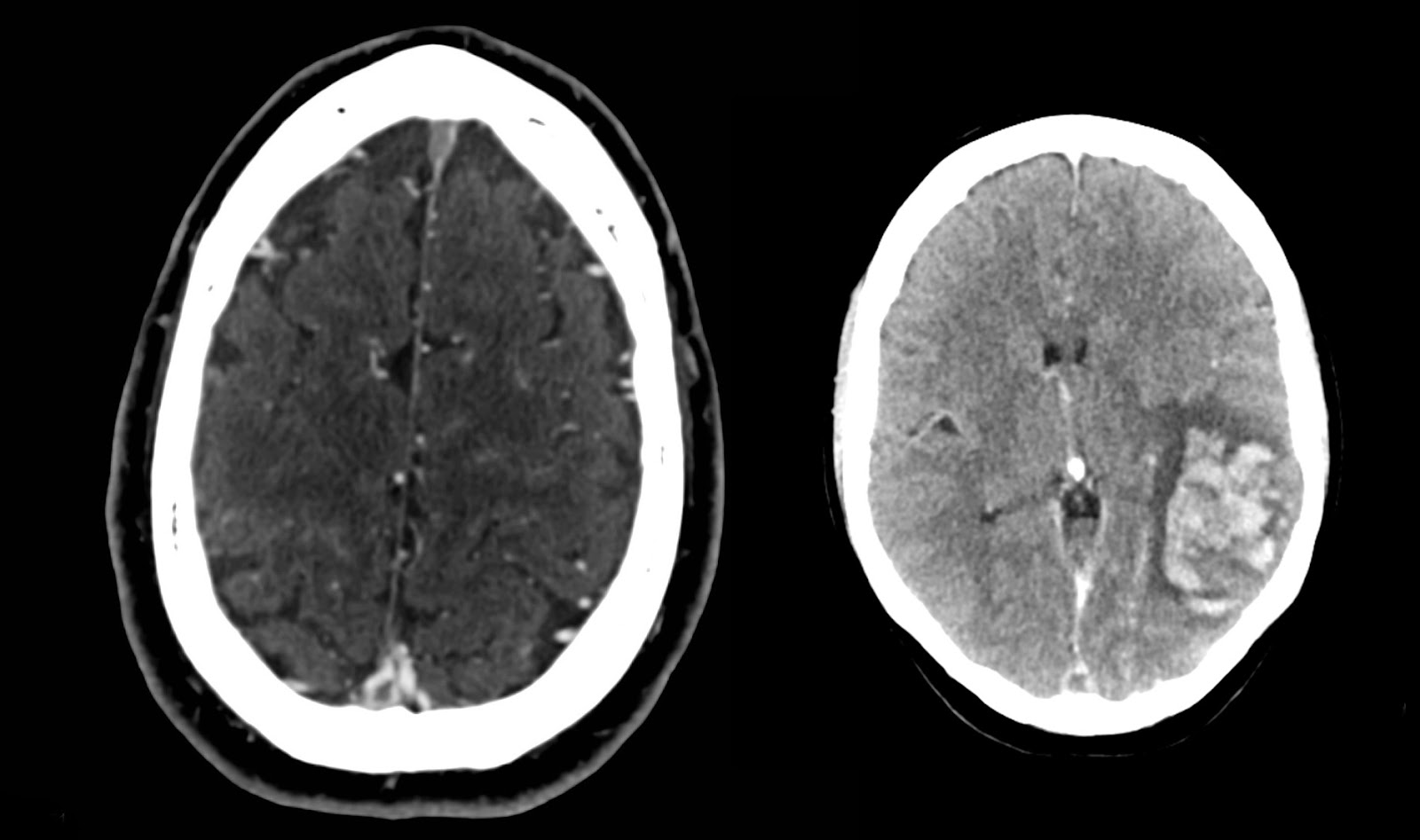
Cerebral venous thrombosis is diagnosed on imaging. There may be clues on a noncontrast CT of the head, such as the dense triangle sign or the cord sign, but the CT will be normal in at least 30% of cases and many of the abnormal findings are nonspecific. MRI is the most sensitive imaging modality, but for most emergency departments the CT venogram will be the first test of choice, with a sensitivity of 95%.
Multiple studies have looked at DDimer as a test for CVT, but the short answer is that it doesn’t work.
Cord sign: A cord-like hyperattenuation within a dural venous sinus.
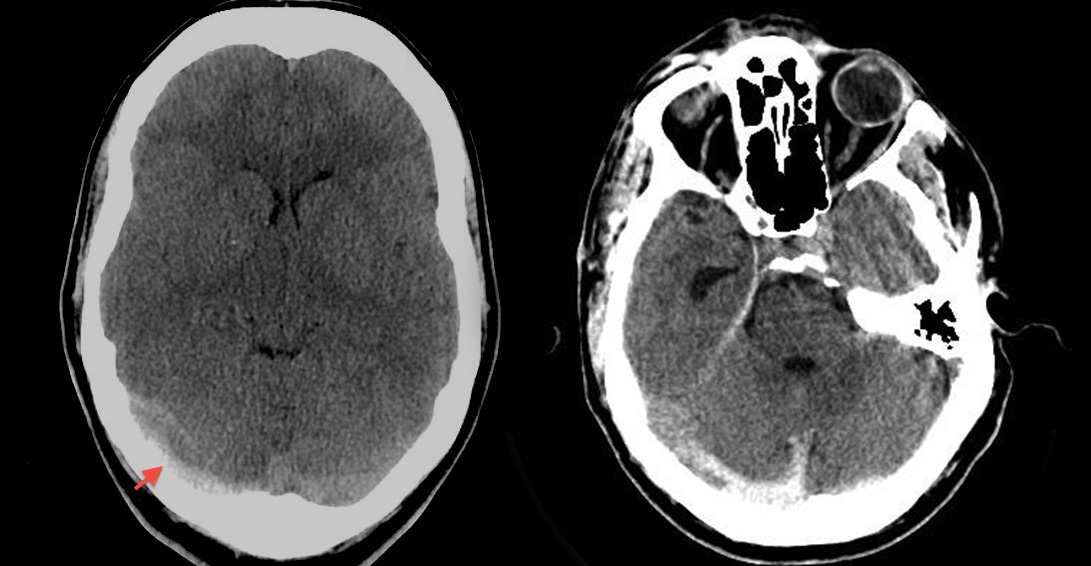
Dense triangle (or vein) sign: A hyperattenuating lesion in one of the veins or sinuses. When it occurs in the superior sagittal sinus, makes a denser triangle at the posterior aspect of the brain.
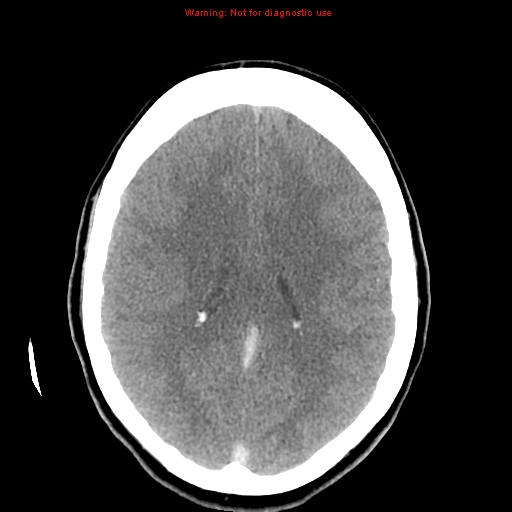
Empty delta sign: A triangular filling defect in the superior sagittal sinus seen on contact CT or MRI.
How is it treated?
Obviously, start with the ABCs. If there is elevated ICP, that needs to be managed. If the patient is having seizures or presents in status epilepticus, treat that first.
The treatment of cerebral venous thrombosis is anticoagulation, even in the presence of hemorrhage. There are two small RCTs that demonstrate better neurologic outcomes and decreased mortality with anticoagulation, without an increase in the rate of intracranial hemorrhage. Long term management has traditionally been with coumadin, with an INR target of 2-3 for 3-6 months if the CVT was provoked, 6-12 months if unprovoked, and lifelong if recurrent. Although some clinicians are using DOACs, there is no evidence for their use at this time.
If the CVT was provoked by an underlying cause, it should obviously be addressed. Anti-epileptics should not be given prophylactically, but should be started if a seizure does occur.
If anticoagulation is ineffective, systemic thrombolytics, endovascular therapy, and surgery have all been attempted.
What is the prognosis?
Prognosis is usually good, with up to 80% of patients making a complete recovery. However, 30 day mortality is about 5%, and about 15% of patients will end up with a severe disability or die. There is about a 5% lifetime chance of recurrence and about half of patients suffer from chronic headaches after a CVT.
Other FOAMed
Cerebral venous sinus thrombosis in the IBCC
Deep cerebral vein thrombosis on Radiopaedia
Morgenstern, J. Cerebral Venous Thrombosis: A rapid review, First10EM, October 19, 2020. Available at:
https://doi.org/10.51684/FIRS.42632


5 thoughts on “Cerebral Venous Thrombosis: A rapid review”
“Oral contraceptives” are not a drug class despite what many emergency physicians seem to think.. You really should ask what kind of OCPs are being used. Estrogen is pro-thrombotic but progesterone has minimal if any thrombotic effect. In fact progesterone only contraception (pills, injections, sub-q and IUDs) are recommended for women who have had DVTs or have underlying thrombophillic states. See ACOG Practice Bulletin #206 ObGyn 133:2 Feb 2019 or the CDC’s USMEC.
You are entirely correct. I tend to use it as a short hand, as typing out “estrogen containing oral contraceptive” every time is annoying, but I hadn’t considered that some clinicians might not be making the distinction. Will change the post to be more specific when I get the chance.
Great post !
I’ve had a handful of these and for that reason have always suspected they are under diagnosed a bit
On the other hand , doing a CT venogram on all young women with progressive headache over a few days with one additional risk factor for VTE? Number needed to scan would be very high – especially if we take the incidence at face-value (the 10-15% maybe even 25% Monosymptomatic headache presentations of the 1/100.000 cases) . And even if you find one in that population , because we are not that sure about how to evaluate pre-test probability , they might as well be false positive (unless they are qualitatively obvious I.e with secondary bleeding ). It’s frustrating because when I have had a case I find it hard to go back and make a general rule out of why I made the decision to scan specifically that particular patient but not her neighbour with headache. And so , I usually say , when people and how to find them, that I truly don’t know how to do it without scanning and over testing a lot of women
The more severe presentations (Seizures, confusion etc) are usually easier to pick up – more about having it on your differential
All the best
Peter
A great support for us to refresh our knowledge regarding these clinical discussions. Thank you very much for your effort.
”Multiple studies have looked at DDimer as a test for CVT, but the short answer is that it doesn’t work”
I and all guidelines have been of the same oppinion , but here the other day I fell over this meta-analysis on isolated headache and CVST . Could be a good article to dissect
Alonso et al, 2015 D-dimer for the exclusion of cerebral venous thrombosis: a meta-analysis of low risk patients with isolated headache https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4517419/pdf/12883_2015_Article_389.pdf
And it doesn’t seem to be part of the most recent (to my knowledge) 2017 guideline from the European Stroke Organization