
We have discussed evidence that antibiotics may not help diverticulitis multiple times on this blog (for example here and here). After another negative RCT, it is time to tackle the difficult question of how much evidence we need to overturn long standing medical practices.
The paper
The STAND trial: Jaung R, Nisbet S, Gosselink MP, Di Re A, Keane C, Lin A, Milne T, Su’a B, Rajaratnam S, Ctercteko G, Hsee L, Rowbotham D, Hill A, Bissett I. Antibiotics Do Not Reduce Length of Hospital Stay for Uncomplicated Diverticulitis in a Pragmatic Double-Blind Randomized Trial. Clin Gastroenterol Hepatol. 2020 Mar 30:S1542-3565(20)30426-2. doi: 10.1016/j.cgh.2020.03.049. PMID: 32240832
The Methods
This was an international, multicenter, placebo-controlled, double-blind, RCT from 4 hospitals in New Zealand and Australia.
Patients
Adult patients admitted to the hospital with CT proven Hinchley 1a (no evidence of perforation, abscess, or peritonitis) uncomplicated acute diverticulitis. Patients were excluded if they had 2 or more SIRS criteria on presentation to hospital. Immunosuppressed patients were also excluded.
All patients were treated with a standardized treatment protocol covering analgesia, antiemetics, diet, and discharge criteria.
Intervention
Antibiotic therapy, with the clinicians choosing between an intravenous regimen and an oral regimen to start.
- IV: intravenous cefuroxime 750 mg every 6 hours PLUS oral metronidazole 400 mg 3 times a day for a maximum of 48 hours, after which patients were changed to the oral regimen.
- Oral: Augmentin [amoxicillin/clavulanic acid] 625 mg 3 times a day for a minimum of 5 days.
Comparison
Placebo.
Outcome
The primary outcome for this study was the length of hospital admission in hours from registration in the emergency department to discharge into the community.
The Results
Out of 459 patients screened for eligibility, 180 were randomized in the trial.
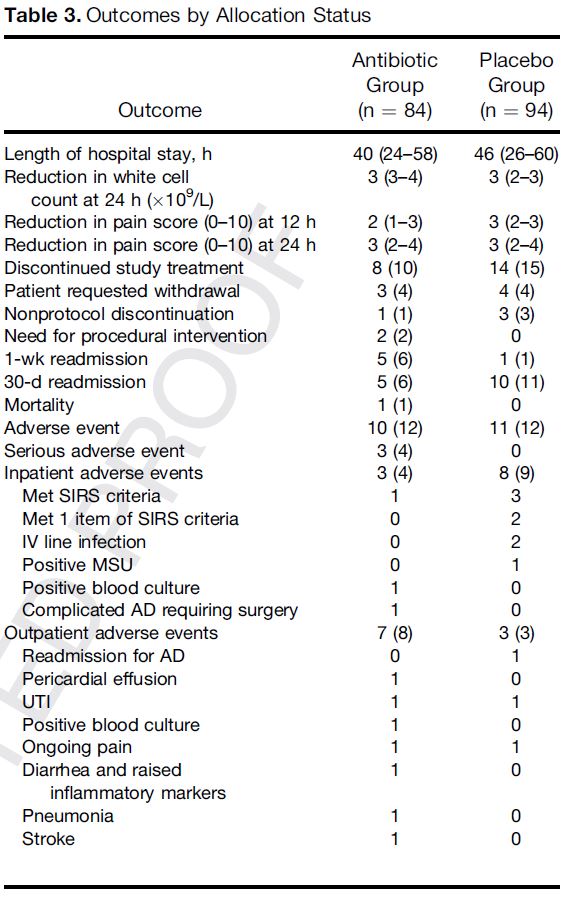
There was no statistical difference in the primary outcome of hospital length of stay. Median length of stay was 40 hours in the antibiotic group (95% CI 24-58) and 46 hours in the placebo group (95% CI 27-60).
There also weren’t any differences in the secondary outcomes. 2 patients needed procedural interventions in the antibiotic group, as compared to 0 in the placebo group. 1 patient in the antibiotic group died as compared to 0 in the placebo group. Readmission within 1 week occurred in 6% of the antibiotic group as compared to 1% of the placebo group. Overall adverse events were exactly equal.
My thoughts
Before getting to the broader question of whether we now have enough evidence to change practice, there are a few significant limitations of this trial to note.
This is a very select subset of diverticulitis patients, but I have a hard time figuring out which way the selection bias pushes the results. On the one hand, these were only the patients that required admission to the general surgery service. Most uncomplicated diverticulitis can be treated as an outpatient, so this study should represent the sickest subset of diverticulitis patients. On the other hand, patients were excluded if they had 2 or more SIRS criteria, so almost all sick patients would have been excluded. Honestly, this is a bizarre group of patients. It is incredibly rare for me to want to chase down the diagnosis of diverticulitis in a patient without SIRS criteria, so I have a hard time understanding who these results should apply to.
Although patients prefer to go home early, length of stay is not a great outcome to use when comparing IV to oral antibiotics, as there are many factors intrinsic to the therapies that will influence length of stay, regardless of whether the patient is getting better. The study wasn’t powered for the most important outcomes, but they actually seem to favour the no treatment group a little bit.
This small trial is clearly underpowered for rare events. These could occur in either group, whether sepsis from an untreated infection or Clostridium difficile from unnecessary antibiotics. At this point I think it clear that there isn’t going to be a huge benefit from antibiotics in uncomplicated diverticulitis, but the precise harms versus benefits are still mostly unknown.
How does this fit with the existing evidence?
To quickly review, like many of our traditional practices in medicine, there doesn’t seem to be a single study that supports antibiotics in diverticulitis. The Cochrane review identified 3 RCTs looking at the topic – only 1 of which compared antibiotics to no antibiotics – and they couldn’t identify any evidence that antibiotics help. (Shabanzadeh 2012) The one RCT was a multicenter trial that included 623 adults with uncomplicated CT proven diverticulitis, and compared broad spectrum intravenous antibiotics (such as piperacillin-tazobactam) to no antibiotics, and found no overall differences. Only 3% of the patients in the no antibiotic group ultimately had to be given antibiotics. (Chabok 2012). There was a subsequent RCT that compared antibiotics to observation in 528 adult patients with CT proven uncomplicated diverticulitis, although this group of patients was allowed to have small pericolic abscesses (Hinchey Ib). (Daniels 2017) The only statistically significant finding in that trial was that antibiotics resulted in a longer hospital stay, but the trial was still underpowered for more important clinical outcomes. As compared to these larger trials, the newer STAND trial doesn’t really add much, but it is always important to see results replicated.
There is also some observational data that followed a group of patients who weren’t given antibiotics, and although there is no comparison group, 98% recovered without any complication. (Isacson 2015) Therefore, even if there is a benefit from antibiotics, we know the benefit must be small, as 98% of patients do well no matter what you do.
A more recent systematic review and meta-analysis that combined RCT and observational data concluded that “the surgical dogma of routine antibiotic use in the management of AUD is long standing and lacks a clear evidence base.” (Tandon 2018) The found no difference in recurrence rate, readmission rate, requirement of surgery during follow‐up, or the need for percutaneous drainage. Antibiotics resulted in longer lengths of hospital stay. The overall quality of evidence is only moderate.
Is it time to change practice?
The answer to this question will depend in large part on your current practice, but even before this most recent RCT, my approach to diverticulitis had changed. These trials suggest that it is not all that important for me to make the diagnosis of uncomplicated diverticulitis. For many well appearing patients with left lower quadrant pain in whom I would have ordered imaging for diverticulitis in the past, I now forgo imaging. I treat the patients’ symptoms, often check some labs, and perform a repeat exam. If there are no indications of complicated disease, I will frequently just treat their symptoms with NSAIDs and a few days of modified diet, whether or not their official diagnosis is diverticulitis. Knowing that antibiotics don’t seem to help, I now reserve the CT for situations where the patient is not improving or appears unwell, to look for complications or an alternative diagnosis.
Based on the lack of evidence, the American Gastroenterological Association Institute guidelines suggest that “antibiotics should be used selectively, rather than routinely, in patients with acute uncomplicated diverticulitis. (Conditional recommendation, low quality of evidence).” (Stollman 2015) Unfortunately, the guideline doesn’t really provide any further advice on what “selectively” means, so it is hard to know who should and shouldn’t be treated. Similar guidelines suggesting more selective use of antibiotics have been released by numerous other organizations. (Andersen 2012; Andeweg 2013; Cuomo 2014; Kruis 2014)
I don’t know exactly how to apply these guidelines, because I don’t know how to be selective in who I treat. Clearly, unwell or immunosuppressed patients get treatment, but otherwise the selection criteria are unclear. For the most part, I try to perform my selection through selective imaging. Most patients don’t get imaging. If the patient was sick enough for me to want to order a CT, they were probably sick enough to get antibiotics – at least for now. However, when I do give antibiotics, I do so as part of a shared decision making process, and despite my recent rant, I even occasionally use a delayed antibiotic prescription for uncomplicated diverticulitis.
Overall, despite significant limitations, the evidence tends to point towards a lack of benefit, and we know that antibiotics have many side effects. The evidence is far from perfect, but you have to make decisions based on what we have. An antibiotics for everyone approach is probably wrong. An antibiotics for no one approach is also probably wrong.
This is evidence based medicine at its finest. Read the studies. Apply your clinical expertise. Then talk to your patients to incorporate their values. This is what makes evidence based medicine so powerful and fun.
Bottom line
This certainly isn’t the last time we hear about this topic. (For example Mora Lopez 2017 is pending). There has never been evidence that antibiotics help in diverticulitis. We now have 3 RCTs and a number of observational trials showing no benefit. If a patient is only going to have mild, uncomplicated diverticulitis, you can probably forgo imaging and just treat the patient symptomatically. In patients sick enough to require imagining, I still treat most of the time, but I have a high bar for imaging, so this is a select group of sicker patients.
References
Andersen JC, Bundgaard L, Elbrond H, et al: Danish national guidelines for treatment of diverticular disease. Dan Med J 2012; 59: C5543.
Andeweg CS, Mulder IM, Felt-Bersma RJ, et al: Guidelines of diagnostics and treatment of acute left-sided colonic diverticulitis. Dig Surg 2013; 30: 278–292.
Chabok A, Påhlman L, Hjern F, Haapaniemi S, Smedh K; AVOD Study Group. Randomized clinical trial of antibiotics in acute uncomplicated diverticulitis. Br J Surg. 2012 Apr;99(4):532-9. PMID: 22290281
Cuomo R, Barbara G, Pace F, et al: Italian consensus conference for colonic diverticulosis and diverticular disease. United European Gastroenterol J 2014; 2: 413–442.
Jaung R, Nisbet S, Gosselink MP, Di Re A, Keane C, Lin A, Milne T, Su’a B, Rajaratnam S, Ctercteko G, Hsee L, Rowbotham D, Hill A, Bissett I. Antibiotics Do Not Reduce Length of Hospital Stay for Uncomplicated Diverticulitis in a Pragmatic Double-Blind Randomized Trial. Clin Gastroenterol Hepatol. 2020 Mar 30:S1542-3565(20)30426-2. doi: 10.1016/j.cgh.2020.03.049. Epub ahead of print. PMID: 32240832.
Daniels L, Ünlü Ç, de Korte N, van Dieren S, Stockmann HB, Vrouenraets BC, Consten EC, van der Hoeven JA, Eijsbouts QA, Faneyte IF, Bemelman WA, Dijkgraaf MG, Boermeester MA; Dutch Diverticular Disease (3D) Collaborative Study Group. Randomized clinical trial of observational versus antibiotic treatment for a first episode of CT-proven uncomplicated acute diverticulitis. Br J Surg. 2017 Jan;104(1):52-61. doi: 10.1002/bjs.10309. Epub 2016 Sep 30. PMID: 27686365.
Isacson D, Thorisson A, Andreasson K, Nikberg M, Smedh K, Chabok A. Outpatient, non-antibiotic management in acute uncomplicated diverticulitis: a prospective study. International journal of colorectal disease. 30(9):1229-34. 2015. PMID:25989930
Shabanzadeh DM, Wille-Jørgensen P. Antibiotics for uncomplicated diverticulitis. Cochrane Database Syst Rev. 2012;11:CD009092. PMID: 23152268
Kruis W, Germer CT, Leifeld L, et al: Diverticular disease: guidelines of the German Society of Gastroenterology, Digestive and Metabolic Diseases and the German Society for General and Visceral Surgery. Digestion 2014; 90: 190–207.
Mora Lopez L, Ruiz-Edo N, Serra Pla S, et al: Multicentre, controlled, randomized clinical trial to compare the efficacy and safety of ambulatory treatment of mild acute diverticulitis without antibiotics with the standard treatment with antibiotics. Int J Colorectal Dis 2017; 32: 1509–1516.
Stollman N, Smalley W, Hirano I, . American Gastroenterological Association Institute Guideline on the Management of Acute Diverticulitis. Gastroenterology. 149(7):1944-9. 2015. PMID: 26453777
Tandon A, Fretwell VL, Nunes QM, Rooney PS. Antibiotics versus no antibiotics in the treatment of acute uncomplicated diverticulitis – a systematic review and meta-analysis. Colorectal Dis. 2018 Jan 11. doi: 10.1111/codi.14013. Epub ahead of print. PMID: 29323778.
Morgenstern, J. Diverticulitis and antibiotics: time to change practice?, First10EM, October 12, 2020. Available at:
https://doi.org/10.51684/FIRS.47583



4 thoughts on “Diverticulitis and antibiotics: time to change practice?”
If there is no evidence favoring your current treatment then is it not logical that any evidence should be embraced and be allowed to change it?
Absolutely. And for many practices in medicine, I have completely abandoned “traditional” practice when it became clear that it was never based on science. However, it can becomes somewhat complex as there are multiple sources of evidence that extend beyond traditional studies, and it isn’t always clear which claim should be given the burden of proof. For diverticulitis, although there are no studies showing benefit, there is physiology and lots of experience that suggests a possible benefit. We now have multiple RCTs showing no benefit, but they are somewhat limited in scope. They certainly aren’t definitive. How one weighs those types of evidence isn’t straight forward, although quality RCTs are always going to be a better source of evidence that observation or physiology. Personally, I self diagnosed myself with diverticulitis 2 years ago, and the only treatment I took was advil. I think some doctors will look at this evidence and completely change practice. Some will be more conservative and wait for more evidence. And many will fall in between, picking and choosing the lower risk patients to avoid antibiotics. I have a hard time criticizing any of these approaches, but the middle ground may make the most sense for a practice so engrained in medicine.
In well appearing infants under 60 days fever above 38.5 C is regarded as a significant inflammatory / infective marker
So .in the older patients fever is subdued but lover 37.5 once or 37.2 twice or 1.1 C above baseline is significant .
So is CRP and ESR and tenderness over diverticulum well appearing and pain .