I don’t think that the concept of “aerosol generating medical procedures” (AGMP) is well supported by scientific evidence. However, this terminology is so widely employed that I will use it throughout this series of posts on high risk medical procedures. The term “AGMP” is really used to identify clinical scenarios in which healthcare workers are at high risk of contracting an infectious disease (currently COVID-19) and may require increased levels of personal protective equipment (PPE). Considering that patients constantly produce infectious aerosols, the actual production of aerosols may be irrelevant, although procedures that significantly increase aerosol production or dispersion may require special attention. At the end of the day, it is not the production of aerosols, but the risk of disease transmission that we really care about.
The evidence surrounding “aerosol generating medical procedures” is generally weak. There are many caveats that need to be considered. Rather than repeat the caveats in every new post, I will refer you to the discussion in the original post. One point that must be emphasized in each post: the burden of proof clearly lies with those claiming that a procedure is safe. For most procedures, the evidence is very weak. Many have used the absence of definitive evidence of harm to claim that there is no harm, and that is inappropriate. We must follow the precautionary principle. If the evidence is inconclusive, we should make the cautious interpretation, especially when healthcare workers are getting sick significantly more often than the general population. The burden of proof lies with the claim that a procedure is safe.
Face-mask oxygen – Bottom line
The best available evidence is that using face mask oxygen is a high risk procedure that may increase the risk of disease transmission to healthcare workers. So long as we are working within the “AGMP” paradigm, an oxygen mask should be considered an “aerosol generating medical procedure”.
There doesn’t appear to be any evidence about the risk from filtered oxygen masks or nasal prongs. The lack of evidence does not in any way prove they are safe.
Evidence for safety
This will sound a little repetitive throughout these posts, but I can find absolutely no evidence to support the contention that the use of facemask oxygen without airborne precautions is safe for healthcare workers.
Evidence for clinical transmission
The best available evidence suggests that facemask oxygen is associated with increased risk to healthcare workers. In one study, the manipulation of an oxygen mask was actually the highest risk factor for healthcare workers to contract SARS, with an odds ratio of 17 (95% CI 1.8-165). (Loeb 2004) Although the systematic review is not statistically significant, the odds ratio is compatible with a significant risk from oxygen mask therapy (OR 4.6 95% CI 0.6-32.5). (Tran 2012) In another case control study from SARS that wasn’t included in the Tran meta-analysis, the use of a high flow oxygen mask was associated with increased transmission of SARS (OR 2.42; 95% CI 1.15-5.08; p =0.02). (Yu 2007) No studies have specifically looked at filtered oxygen masks. I also couldn’t find any studies looking at the transmission risk of nasal prongs.
Bottom line: Although observational data always has weaknesses, the best available evidence clearly suggests that use of face mask oxygen increases the risk of disease transmission.
Evidence of aerosol production and spread
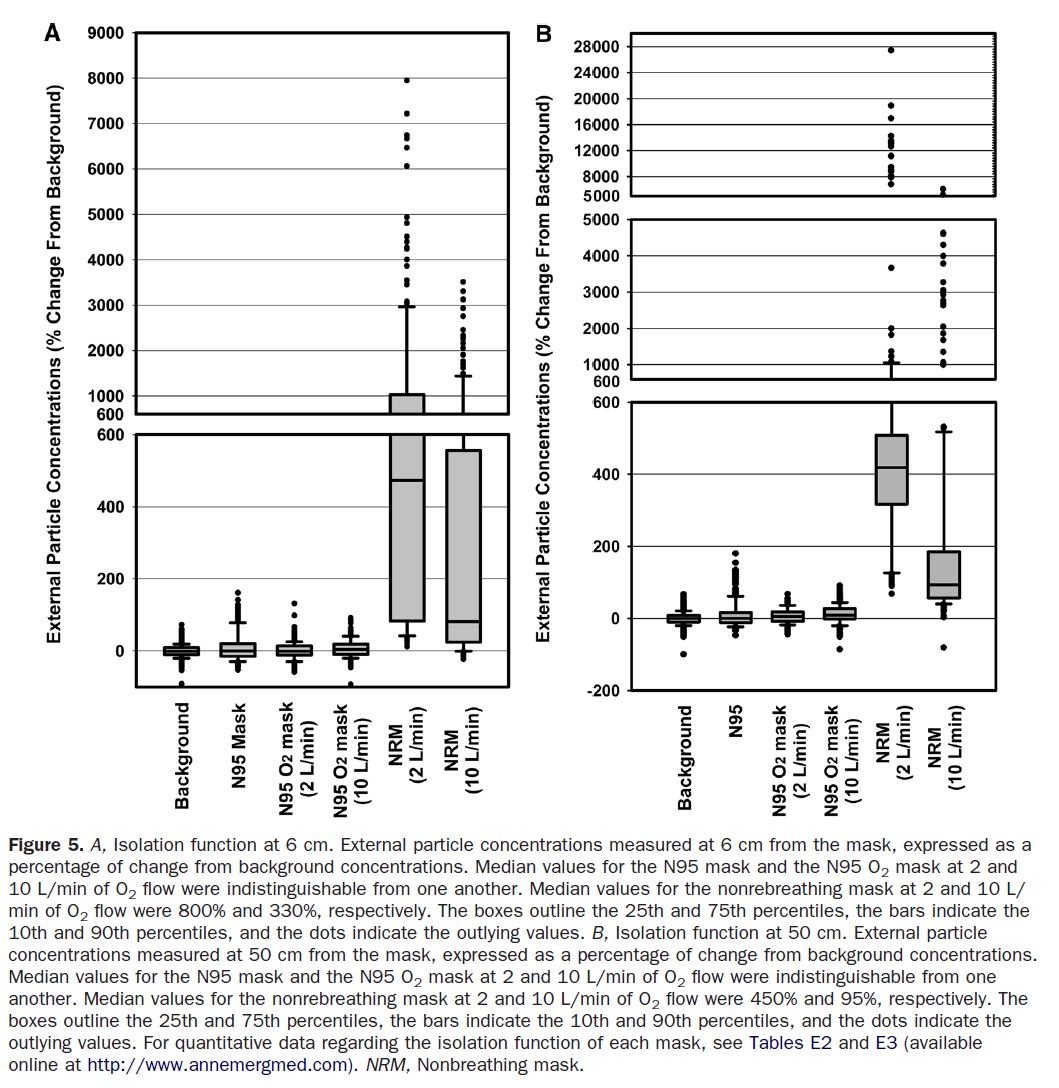
It is not clear that face mask oxygen actually ‘generates’ aerosols, but it has the capacity to disperse them further, which probably increases infectious risk. One study did not see an increase in aerosols after oxygen mask application, but the aerosol counts at baseline were already in the millions per cubic meter, so a small increase might not have been noticed. (Simmonds 2010) (Once again, patients produce aerosols even without procedures.) In contrast, another laboratory controlled study found a very significant increase in airborne particle concentrations when an oxygen mask was used (a mean 800% increase at 6cm from the patient and 450% increase at 50cm at just 2 L/min flow, with some outlying patients with massive total increases in aerosols). Unfortunately, although this study measured oxygen delivery with the HiOx mask, it didn’t measure aerosol generation for some reason. (Mardimae 2006)
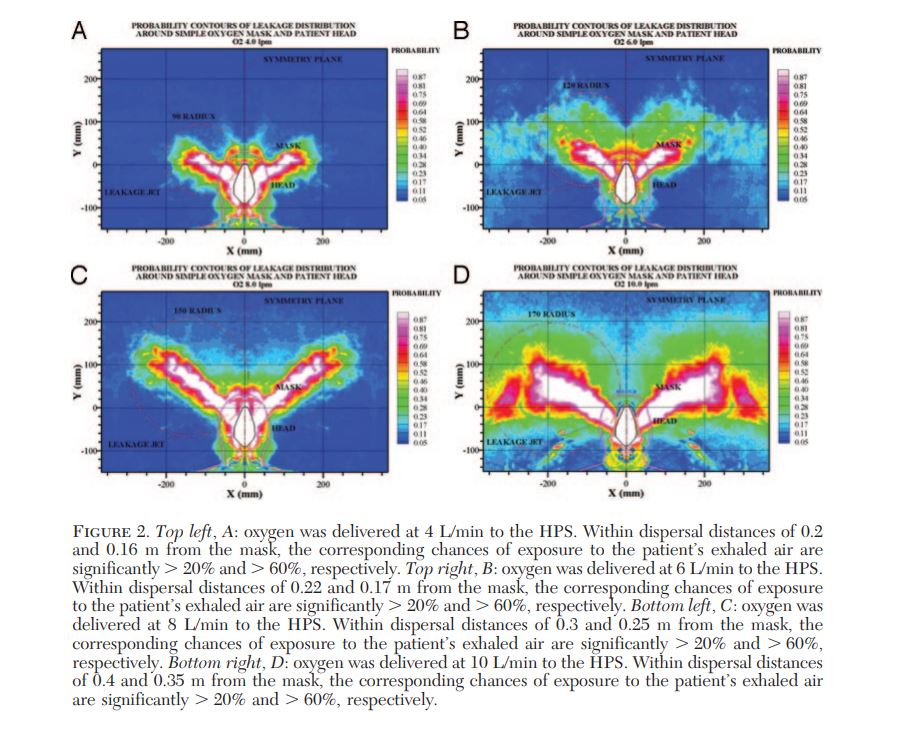
Oxygen masks cause increased dispersion of visual droplets and smoke, with higher oxygen flows leading to greater dispersion. Most air exits the exhalation ports, but there is also significant leak around the edges of the mask (which will limit the value of filters on the exhalation ports). (Hui 2007; Hui 2014; Ip 2007)
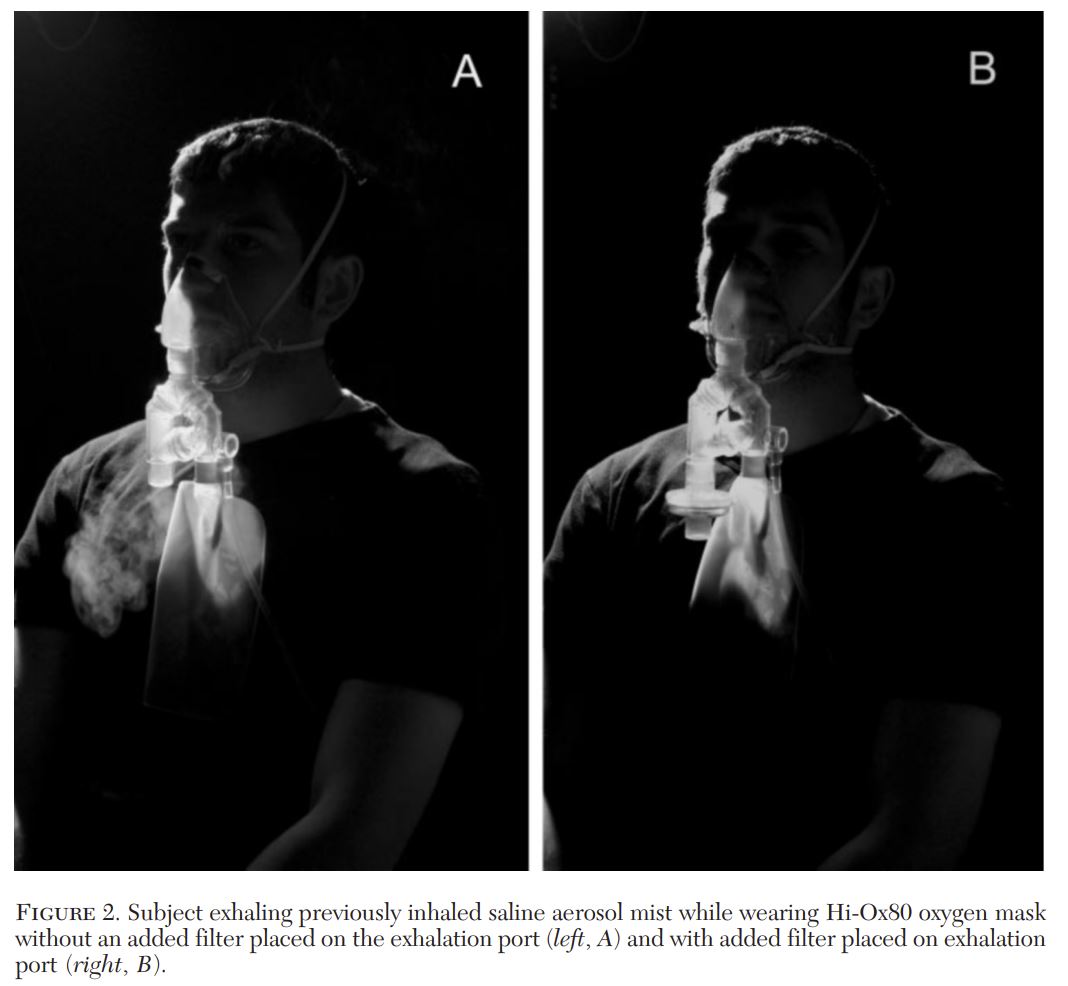
The addition of a viral filter to an oxygen facemask has unclear impacts. They should theoretically be better, but their benefits are also significantly limited by the significant leak that will occur around the edges of the mask, especially at higher flow rates. In a well fitting HiOx mask, there is some qualitative evidence of decreased aerosol dispersion. (Somogyi 2004) However, this study is extremely limited, as the mask wasn’t actually hooked up to oxygen, which would significantly increase leak and aerosol dispersion.
Nasal prongs will also increase aerosol dispersion (in simulated studies using smoke as a marker). (Hui 2014)
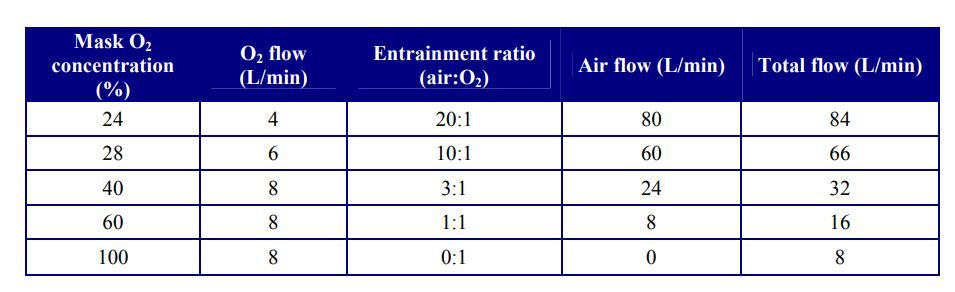
I don’t use Venturi masks in the emergency department, but it is worth remembering that lower oxygen rates actually results in significantly higher total air flow rates.
Discussion
I don’t understand how it is possible that so many hospitals have classified face mask oxygen as non-aerosol generating when there is a study that showed a statistically significant increase in transmission of SARS with an odds ratio of 17! We don’t even need the precautionary principle to know that precaution is needed.
Far too many “evidence based” guidelines made the definitive statement that facemask oxygen was not an aerosol generating procedure based on inappropriate interpretations of the Tran meta-analysis. (tran 2012) In the Tran meta-analysis, facemask oxygen had an odds ratio of 4.6 for increased transmission of disease. It wasn’t statistically significant, but it is completely inappropriate to use the lack of statistical significance as proof that there is no risk. Every available study had an odds ratio consistent with risk, and 2 of the 3 studies were statistically significant. We can talk about the weakness of the data, but the only appropriate conclusion from these studies is that the use of facemask oxygen was a risk factor in the transmission of SARS to healthcare workers.
The use of oxygen masks with viral filters is relatively new to most of us. Although they make sense, there is no good evidence that they decrease risk of disease transmission. They should probably be preferred over standard nonrebreathers, but they should not be used as a replacement for appropriate PPE, which based on this data is clearly airborne precautions when facemask oxygen is being used.
There is almost no data to guide us when it comes to nasal prongs. Unfortunately many IPAC guidelines have overlooked the most basic of science rules: absence of evidence is not the same as evidence of absence. Based on basic physics, nasal prongs are probably lower risk than oxygen masks. On the other hand, at least the oxygen mask covers the patient’s mouth and nose. When the patient’s surgical mask comes off, which it almost inevitably does, the nasal prongs may actually be higher risk than oxygen masks because they distribute aerosols without the barrier provided by the mask.
None of this data is definitive. Given the prevalence of COVID-19 worldwide right now, it would not be hard to generate much better data than we currently have. Unfortunately, such studies are likely hindered by the dogmatic guidelines that currently shape IPAC practices. However, it is completely clear that there is no data to suggest that the use of facemask oxygen is safe, and until we have that data we must rely on the precautionary principle and classify facemask oxygen as a “aerosol generating medical procedure”.
Other FOAMed
The original AMGP evidence review
COVID-19 is spread by aerosols: an evidence review
“Aerosol Generating Medical Procedure” is a faulty paradigm
Note: I will attempt to update this post whenever new evidence becomes available. If there are any studies you think I missed, or anything you think I got wrong, please comment below. The goal, as always, is to have the most accurate understanding of the science to help guide our clinical practice.
References
Loeb M, McGeer A, Henry B, et al. SARS among critical care nurses, Toronto. Emerg Infect Dis. 2004;10(2):251–255. doi:10.3201/eid1002.030838 PMID: 15030692
Hui DS, Hall SD, Chan MT, et al. Exhaled air dispersion during oxygen delivery via a simple oxygen mask. Chest. 2007;132(2):540–546. doi:10.1378/chest.07-0636 PMID: 17573505
Hui DS, Chan MT, Chow B. Aerosol dispersion during various respiratory therapies: a risk assessment model of nosocomial infection to health care workers. Hong Kong Med J. 2014;20 Suppl 4:9–13. PMID: 25224111
Ip M, Tang JW, Hui DS, et al. Airflow and droplet spreading around oxygen masks: a simulation model for infection control research. Am J Infect Control. 2007;35(10):684–689. doi:10.1016/j.ajic.2007.05.007 PMID: 18063134
Simonds AK, Hanak A, Chatwin M, et al. Evaluation of droplet dispersion during non-invasive ventilation, oxygen therapy, nebuliser treatment and chest physiotherapy in clinical practice: implications for management of pandemic influenza and other airborne infections. Health Technol Assess. 2010;14(46):131–172. doi:10.3310/hta14460-02 PMID: 20923611
Somogyi R, Vesely AE, Azami T, et al. Dispersal of respiratory droplets with open vs closed oxygen delivery masks: implications for the transmission of severe acute respiratory syndrome. Chest. 2004;125(3):1155–1157. doi:10.1378/chest.125.3.1155 PMID: 15006983
Tran K, Cimon K, Severn M, Pessoa-Silva CL, Conly J. Aerosol generating procedures and risk of transmission of acute respiratory infections to healthcare workers: a systematic review. PLoS One. 2012;7(4):e35797. PMID: 22563403
Yu IT, Xie ZH, Tsoi KK, Chiu YL, Lok SW, Tang XP, Hui DS, Lee N, Li YM, Huang ZT, Liu T, Wong TW, Zhong NS, Sung JJ. Why did outbreaks of severe acute respiratory syndrome occur in some hospital wards but not in others? Clin Infect Dis. 2007 Apr 15;44(8):1017-25. doi: 10.1086/512819. Epub 2007 Mar 9. PMID: 17366443
Morgenstern, J. An oxygen mask is an “AGMP”, First10EM, December 9, 2020. Available at:
https://doi.org/10.51684/FIRS.52391