Morgenstern, J. Subarachnoid Hemorrhage: What is the role of LP?, First10EM, September 21, 2020. Available at:
https://doi.org/10.51684/FIRS.42400
Headache is a very common presenting complaint in emergency medicine, and most patients have a benign cause. (Davenport 2002) However, approximately 1% of patients will be diagnosed with a subarachnoid hemorrhage. (Goldstein 2016; Carpenter 2016) Subarachnoid hemorrhage has a high mortality, with 25% of patients dying within 24 hours and up to 50% dying within 3 months. Among survivors, 30-50% will experience some form of disability and half will never return to work. (Davenport 2002; Carpenter 2016) Historically, we have taught that a lumbar puncture is required after a negative CT scan to effectively exclude the diagnosis of subarachnoid hemorrhage, but the value of this approach has been questioned. This post is going to go through a large quantity of evidence to make us all experts in the diagnosis of subarachnoid hemorrhage. (This started as a quick post on the newest paper from the Perry group, and rapidly transformed into a beast. You might want to digest it over more than one sitting.)
What are the signs and symptoms of subarachnoid hemorrhage?
To diagnose subarachnoid hemorrhage (SAH), we need to know how SAH presents. When patients present with altered mental status or focal neurologic deficits, the path forward is not complicated. These patients need a work up, which will almost always include imaging, and will often proceed to lumbar puncture. When patients present with an isolated headache, but alert and neurologically intact, it is more difficult to know who requires further investigation.
There is an excellent systematic review and meta-analysis by Carpenter and colleagues (2016) looking at the diagnosis of subarachnoid hemorrhage. In the studies they identified, the prevalence of SAH ranged from 0.9% to 68% (so selection bias clearly influenced the results of some of the underlying studies). No single element of the history had a very high positive likelihood ratio, but subjective neck stiffness did increase the likelihood of SAH (positive likelihood ratio 4.12 95% CI 2.24-7.59). Onset of the headache over more than 1 hour essentially excludes the diagnosis (negative likelihood ratio 0.06 95% CI 0-0.95). The lack of “worst headache of life” might also decrease the likelihood (LR- 0.36 95% CI 0.01-14.22), although the confidence intervals are huge and not very convincing. In terms of physical exam, neckstifness was associated with SAH (LR+ 6.59 95% CI 3.95-11), but there were no physical exam findings with effective negative likelihood ratios. (Carpenter 2016)
Those numbers aren’t overly encouraging. Exploring the numbers in our largest observational data sets (the Ottawa SAH rule derivation and validation studies), you can see why. Although the average presentation of SAH looks quite different from the average benign headache, no individual aspect is particularly sensitive nor specific. For example, almost all patients with subarachnoid hemorrhage describe their headache as “the worst in their life”, but so do a very large number of patients with benign headaches. Subjective neck stiffness occurs in 75% of SAH, but also occurs in 30% of benign headaches, and because benign headaches are much more common, the finding doesn’t necessarily discriminate. In the table below, I list approximately how common various findings are in both SAH and benign headaches, based on the Perry studies. (Perry 2013; Perry 2017)
| Finding | Patients without SAH | Patients with SAH |
|---|---|---|
| Average age | 44 | 55 |
| Arrive by ambulance | 25% | 60% |
| Onset during exertion | 10-15% | 20% |
| Onset during sex | 6-10% | 5-10% |
| Awoke from sleep | 17% | 10% |
| Thunderclap | 60% | 85% |
| Worst of life | 75-80% | 94-99% |
| Loss of consciousness | 5% | 10% |
| Vomiting | 25% | 65% |
| Neck stiffness on history | 35% | 75% |
| Limited neck flexion (physical) | 4% | 20-30% |
There are some common misconceptions worth noting. A headache that awoke the patient from sleep was actually more common in the benign headache group than the SAH group. Onset during sexual activity was essentially identical in both groups, as was onset during exertion.
Ultimately, I am focusing on headaches with a very rapid onset, especially in somewhat older patients. If it took longer than 1 hour for the headache to reach peak intensity, I am done. If the headache isn’t severe, there would have to be other significant factors to make me consider SAH. Otherwise, no feature is accurate enough to influence my decision to order a CT, but if there are enough worrisome features, they factor into my decision whether to suggest lumbar puncture after a negative head CT.
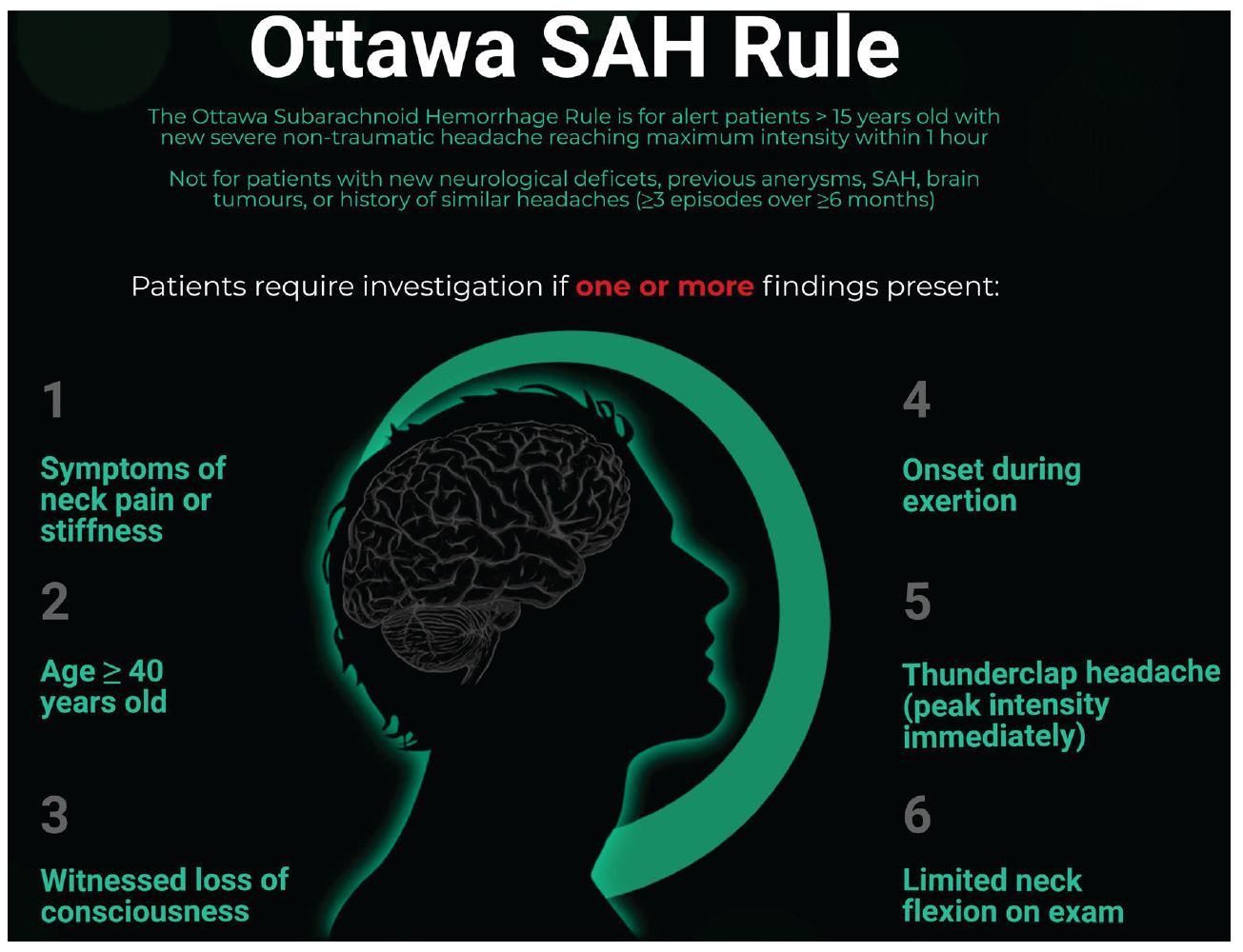
What about this subarachnoid hemorrhage rule?
The Ottawa subarachnoid hemorrhage rule was initially derived as 3 rules. (Perry 2010) Those 3 rules were then validated, but then a fourth rule was created because none of the 3 were perfect. (Perry 2013) The same group revalidated that fourth rule (Perry 2017) and the rule was also externally validated in two chart reviews. (Bellolia 2014; Chu 2018) Finally, the rule was assessed in a before and after implementation study. (Perry 2020)
The end result is a rule with a very high sensitivity (100% with a 95% confidence interval that extends to about 95-97%) but a very low specificity (between 7.5 and 15%). This results in an excellent negative likelihood ratio (0.02) but a dismal positive likelihood ratio (1.17). Like many of the highly sensitive but non-specific rules we have, whether this helps patients will depend a lot on the patient populations it is applied to. If you only apply the rule after you have already decided to order a head CT, it might slightly reduce the need for imaging. However, if the rule was applied widely, or the exclusion criteria are ignored (it doesn’t apply in patients with recurrent headaches), this rule has the ability to massively increase investigation without helping patients.
I really dislike the way the authors have phrased the rule, stating that “patients require investigation if one or more of the findings is present”. This is incorrect. The rule doesn’t increase your likelihood of having SAH at all, with a positive likelihood ratio of only 1.17. It should never be used to drive imaging. The rule would be more acceptable to me if it stated, “investigation should not occur if the patient has none of these findings.”
These studies are incredible efforts, but as always imperfect. The results may be skewed by partial verification bias, in that not every patient received the same gold standard test. A fairly large number of eligible patients who should have been enrolled were missed in these trials, although they look much like the patients who were enrolled based on the demographics. There were also some patients lost to follow up, which could make the numbers look much worse if there were any with missed SAH. When examined in other populations, the rule seems to apply to a very small number of patients, and only about 5% of patients could have SAH ruled out on the basis of the rule, so the clinical utility is limited. (Chu 2018; Bellolia 2014)
In an implementation study, the SAH rule looked somewhat promising. (Perry 2020) It had a sensitivity of 100% (95% CI 98.1-100%), and was associated with a decreased use of lumbar puncture (39% vs 26%). However, everyone in both groups was already essentially following the rule (78% of the “control phase” doctors followed the SAH rule, compared to 86% in the intervention phase). With groups so similar in practice, it is unlikely that the decrease in LPs was a result of the rule. We were already performing fewer LPs with time (based in large part on the work of this group), especially after early head CTs. My guess is that most of the decrease in LPs was happening anyway, and would have also been seen at a control hospital, if one had been included.
Personally, outside of teaching, I don’t see much of a role for this rule. If the exclusion criteria were strictly followed, and it was only considered after the clinician had already made the decision to order a CT, there may be the occasional patient with none of the features in whom the CT could be avoided. (However, if you have a young patient with none of these features, why are you considering SAH in the first place?)
Is the CT within 6 hours really 100% sensitive?
No, it is not.
The study that got everyone excited about a possible 100% sensitivity was a prospective observational trial of 3132 alert adult patients with an acute headache (peak within 1 hour), of whom 7.7% were ultimately diagnosed with SAH. (Perry 2011) Overall, CT scan was 92.9% sensitive, but in the 953 patients in whom the CT was done within 6 hours, they reported a sensitivity of 100%. Unfortunately, there are a number of reasons to think that the 100% number is incorrect. First, the vast majority of these patients didn’t receive a gold standard test. They were followed clinically for 6 months, but it is clearly possible that some patients had a missed aneurysmal SAH, but simply didn’t rebleed in the subsequent 6 months, or were missed by the study’s follow up methods. (They didn’t identify a single case of missed SAH resulting in death or an unscheduled visit in this cohort, which is either very reassuring, or indicates imperfect follow-up.) Furthermore, many of the CTs were reported after the lumbar puncture results were back and available to the reporting radiologist, which could easily have biased the CT report. Indeed, there were 4 patients who were initially sent home with preliminarily normal CTs that were subsequently overread as showing SAH. Finally, even if you accept the point estimate of 100%, it is essentially to recognize the 95% confidence interval, which extends down to a sensitivity of 97%.
The Perry group has subsequently done an implementation study (of both the 6 hour CT and of their SAH rule). (Perry 2020) It is a prospective, multicenter before and after study that included 3672 adult patients with acute onset headache. 1204 patients presented within 6 hours, and 5 had SAH that was missed on CT, resulting in a sensitivity of 95.5% (95% CI 89.8-98.5). Two of these may not have truly been SAH (there was an aneurysm and a presumed traumatic LP). Of the 3 real misses, one was a non-aneurysmal bleed, one was a misread by the radiologist, and one patient with a true aneurysmal SAH was severely anemic, explaining the false negative CT. However, this data makes it pretty clear that a CT scan, even if it is within 6 hours, is not 100% sensitive for SAH.
A systematic review that identified 5 trials (including the first but not the second Perry paper) encompassing 8907 patients concluded that a CT scan within 6 hours of headache onset has a sensitivity of 98.7%. (Dubosh 2016) There were 13 misses out of 8907 patients, or about 1.5 misses per 1000 patients.
In all these studies, there are instances in which CTs were initially read as negative, including by general radiologists, and then later over-read as positive. (Dubosh 2016) This is a significant limitation, and indicates that the reported sensitivity may be lower outside of study settings, especially in community settings where neuroradiologists are not available.
The fallibility of the initial radiology read is confirmed in a study by Mark and colleagues (2016) in which 18 patients were diagnosed with SAH after a negative CT. These 18 scans were then reviewed by neuroradiologists, and they thought that there was evidence of blood on half of the initial CTs. Unfortunately, most of us work in places where scans will never be looked at by neuroradiologists, so the numbers seen in studies may never apply in the community setting.
Bottom line: CT within 6 hours is clearly not 100% sensitive, and the numbers reported in these trials are likely to be better than the numbers we will see in daily community practice.
Is the CT with 6 hours good enough?
Almost certainly.
A perfect test is fool’s gold. Tests with 100% sensitivity don’t really exist, but we don’t need 100% sensitivity for a test to be good enough. The question isn’t whether the CT will be perfect, but whether it will get the post-test probability low enough to eliminate the need for further investigations.
In patients with a true thunderclap headache presenting within 6 hours, the prevalence of subarachnoid hemorrhage appears to be between 7 and 10% (Perry 2011: 7.7%; Perry 2019: 9.2%) The negative likelihood ratio of a CT within 6 hours is 0.01. (Dubosh 2016) Thus, after a negative CT scan, the chance that a patient with a thunderclap headache has a subarachnoid hemorrhage is less than about 0.2%. (Dubosh 2016)
How does lumbar puncture perform in a group of patients with a pretest probability of 0.2%? Not well. I will go through some numbers below, but considering the rate of traumatic taps is usually reported as more than 10%, you will never find the 0.2% needle in that haystack.
People often frame the debate as routine LP versus no LP; LP everyone versus LP no one. Although that makes for a cleaner debate, it isn’t based in reality. Even before Perry’s 6 hour CT study, many patients were not getting a lumbar puncture. In the Perry (2011) study, only half of patients received an LP after a negative CT, and that is in a setting where the physicians knew they were being monitored. We have never lumbar punctured all these patients. The decision to proceed with the more invasive test has always involved physician judgement, and hopefully patient values as well.
Bottom line: Although CT within 6 hours is not 100% accurate, it results in a very low posttest probability.
What if the CT happened after 6 hours?
CT is much less accurate after 6 hours, with a reported sensitivity of approximately 86% (95% CI 78.3-90.3). (Perry 2011) (Backes 2012 reports a 92% sensitivity.) However, we have to be very cautious in interpreting this number. Of 2179 patients who had a negative CT performed after 6 hours, only 119 had a LP performed, and 17 of those lumbar punctures were positive (only 6 needed neurosurgical intervention). 17 misses in 119 patients sounds bad, but it wasn’t 17 misses in 119 patients. We are dealing with significant selection bias here, as only a small number of patients actually had an LP performed. It was actually 17 false negative CTs in 2179 patients, or 0.8%. When framed that way, although this is somewhat worse than the miss rate within 6 hours, it isn’t bad at all, and it looks even better if you only consider the aneurysmal subarachnoid hemorrhages. On the other hand, we are also dealing with partial verification bias here, in that the vast majority of these patients did not receive the gold standard test, so the miss rate could actually be higher. Finally, spectrum bias also probably plays a role. Because of the severity of symptoms, patients with SAH tend to present early, so the incidence of SAH actually decreases in patients presenting after 6 hours. For example, in the Perry 2020 study, the incidence of SAH in patients presenting under 6 hours was 9.1%, whereas the incidence in those presenting after 6 hours was only 3.1%.
The numbers from the Perry 2011 study are imperfect, but they still provide a lot of valuable information. A CT after 6 hours is worse than a CT within 6 hours. (It is unlikely that 6 hours is a magical cutoff. Earlier is better.) However, a negative CT after 6 hours still has a tremendous negative predictive value in this relatively high risk cohort. The post-test probability of having SAH after a negative CT was only 0.8%, or 1 in 125. (And the number is probably even lower than this, as most of these patients did not have aneurysmal bleeds.)
In one retrospective chart review of 2248 patients who had an LP performed to rule out subarachnoid hemorrhage, 67% were negative, 29% were inconclusive or uninterpretable, and 4% were considered positive. However, only 0.4% (9 out of 2248) of patients were found to have a vascular abnormality, and only one of those patients had their CT performed within 6 hours of the headache onset. Ignoring the timing of the CT, a 0.4% positive rate means that we need to perform 250 LPs to identify a single patient with a subarachnoid hemorrhage who required an intervention. For that single true positive LP, there will be 73 with inconclusive or uninterpretable results. (Sawyer 2015) (Because of the various limitations of chart review methodology, these numbers are probably overly optimistic. For a full critical appraisal of this article, check out the SGEM episode.)
Finally, it is clear that lumbar puncture after a negative CT is nowhere close to a standard of care. Only 5% of patients who presented after 6 hours had a lumbar puncture performed after their negative CT. (Perry 2011) There were no obvious bouncebacks. Clearly, physicians are already using judgement in deciding who needs an LP, and we seem to be doing a good job.
Bottom line: CT after 6 hours is not perfect, and there is probably a role for occasional lumbar puncture, but it clearly isn’t necessary in everyone.
Are you using the right CT?
The CT protocol is often somewhat opaque to us in the emergency department. Most places are probably using the same standards used in these studies, but it might be worth checking with your radiologists. I didn’t know that different thickness slices should be used for the posterior fossa, for example. Most of these studies used third generation multi-slice scanners, with 2.5-5 mm slices through the posterior fossa and 5-7.5mm slices for the rest of the brain. (Perry 2011)
More concerning for most of us in the community is the training of the radiologist available. All these studies used specialist neuroradiologists. There were multiple cases in which an initial read was negative, but an overread by a neuroradiologist indicated SAH. (Dubosh 2016) I think that might be a big problem for those of use that work in the community.
What exactly are you looking for on LP?
Red cells
The lumbar puncture debate would be a lot easier if the test always gave us a precise answer. Sure, some lumbar punctures are difficult, and they always take a bit of time, but emergency physicians love procedures. Unfortunately, the results of the LP are too often uncertain. We are searching for blood, but “traumatic taps”, where blood is introduced into the needle from somewhere outside of the CSF, occur in 10-30% of lumbar punctures, although the exact number is highly dependent on the definition of ‘traumatic tap’. (Gorchynski 2007) So how do we interpret the CSF red blood cell number?
The best answer probably comes from a secondary analysis of the Perry 2011 SAH study, in which they looked at just the subset of patients who underwent LP, comparing the CSF results between those with and without a diagnosis of aneurysmal subarachnoid hemorrhage. (Perry 2015) They state that they are not concerned about perimesencephalic bleeds or other non-aneurysmal bleeds, as they generally only require observation and have a good prognosis. In their study, there were 641 patients with abnormal lumbar puncture results, but only 15 of these (2%) were diagnosed with aneurysmal subarachnoid hemorrhage. (This really highlights the number of false positives and difficulties in interpreting LP results.) They found that the combination of a lack of xanthochromia and a red cell count less than 2000×10^6/L in the final tube collected was 100% sensitive (95% CI 74.7-100%) for SAH. Obviously, the confidence intervals are a little concerning, and the specificity isn’t perfect. Only 15 of the 70 patients with these high risk criteria (23%) actually had SAH. Furthermore, the excellent sensitivity is only obtained when combining the red cell count with xanthochromia. On its own, the red cell cut off of 2,000 only had a sensitivity of 93% and a specificity of 91%.
In a chart review of 594 patients who underwent LP for their headache in the ED, 299 had RBCs in their CSF, and SAH was diagnosed in 11 (3.7%). (Gorchynski 2007) In the group with SAH, there were a mean of 399,277 RBCs in tube 1 and 307,700 in tube 4. In the group with a traumatic tap, there were 6763 RBCs in tube 1 and 443 in tube 4. These numbers seem far apart, but unfortunately there is an area of overlap. No patients with a tube 4 RBC count less than 500 was diagnosed with SAH (100% sensitivity) and every patient with a tube 4 RBC count over 10,000 was diagnosed with SAH (100% specificity), but the numbers in between were imperfect. That being said, the vast majority of traumatic taps had RBC counts less than 500, so a cutoff of 500 could still be very helpful in ruling out SAH.

Bottom line: We will likely never find a perfect cutoff, but I find these numbers pretty reassuring. I wouldn’t use the 2,000 RBC threshold as a black and white rule (if a patient has a perfect story and a red cell count of 1900, I am still concerned), but I think it is a reasonable cutoff to use for most patients, as long as it is combined with assessment of xanthochromia. It looks like most traumatic taps will have RBC counts below 500. There is clearly a grey area in between in which the occasional patient will require further workup with a CT angiogram.
Xanthochromia
What exactly is xanthochromia and how accurate is it for the diagnosis of SAH?
One of the big issues with xanthochromia is that it is measured differently in different parts of the world, which makes comparisons difficult. In most hospitals in North America, xanthochromia is simply measured by visual inspection of the CSF. There is a technique to quantitatively measure the colour of CSF (spectrophotometry) which sounds like it should be more accurate, but doesn’t seem to be. Compared to a (rather imperfect) gold standard of angiography and clinical follow-up, visual inspection for xanthochromia has a sensitivity of 84%, specificity of 96%, positive LR of 14.1 and negative LR of 0.35. Spectrophotometry is not any better, with a sensitivity of 87%, specificity of 86%, positive LR of 6.6 and negative LR of 0.29. (Chu 2014) Similar numbers are reported in the Carpenter 2016 meta-analysis. (The sensitivity for a specific type of spectrophotometry is listed as 100%, but the 95% CI extends all the way down to 59%). The studies here aren’t great, but neither are the test characteristics. (Previously discussed in the Articles of the Month.)
Xanthochromia requires up to 12 hours to develop, so can be falsely negative if the LP is performed too early, and can also be falsely positive because of hemolysis. (Carpenter 2016) It is unclear to me how this affects management, but holding patients just so that a lumbar puncture can be done after 12 hours seems impractical. For now, if an LP is needed, I just do it right away, whatever the timing. (I couldn’t find any solid evidence that says we should delay the LP beyond 12 hours, but if you know of studies, please comment below.)
I have always wondered, why not just directly measure the chemicals that make the fluid yellow? I mean, every lab has the capacity to measure bilirubin. Why don’t we just send CSF for bilirubin? Some studies (ie Blok 2015) report their spectrophotometric analysis as a measure of bilirubin, but I have not seen a study where it was directly measured. Can anyone explain that to me?
What are the harms of LP?
I love performing lumbar punctures, but I have to admit that they are a harmful procedure. (All medical interventions are harmful, which is why we really need to stop saying “do no harm”.) There is the pain of the procedure itself. There is the dreaded post-LP headache, which occurs in up to 15% of patients. (Seupaul 2005) Of course, we can reduce this risk by using atraumatic needles, but headaches still occur in about 4% of patients, and they can be quite debilitating. (Nath 2018) There is the time it takes to perform the procedure, prolonging patient stays and taking attention away from other patients in the department. There are a number of rare but serious adverse events, such as epidural hematomas and infections. And perhaps the biggest problem of all is the high number of false positives or traumatic taps that render the procedure unhelpful and provoke further testing (usually a contrast CT angiogram) with its own harms.
What are the harms of missing a subarachnoid hemorrhage?
The fear is that we are going to miss a ‘sentinel bleed’ and that the patient will have a subsequent bleed with significant morbidity or mortality. Although many sources suggest that the risk of missing SAH is incredibly high, most studies I have seen suggest that only a minority of patients (approximately 10%) actually return with a bad outcome.
In one database study that included 1603 patients with a diagnosis of non-traumatic subarachnoid hemorrhage, about 10% had visited an emergency department in the 2 weeks prior to their admission, and 5% had what the authors considered a missed diagnosis in the ED. However, those with a missed diagnosis had a much better prognosis. The missed group had a 6% mortality rate, as compared to the 34% mortality seen in the cohort where the correct diagnosis was made. (Vermeulen 2007)
In another chart review of 450 patients with SAH, 12% were considered misdiagnosed on first medical contact. (Kowalski 2004) Overall, the group misdiagnosed did better than the group that was diagnosed on first visit, but obviously the diagnosed group was much sicker. After they try to adjust for that fact, the misdiagnosed group looks like they have higher mortality and worse neurologic outcomes, but there are almost certainly confounders that make this adjustment inaccurate.
Clearly we don’t want to miss SAH, but no one is trying to. I don’t find this data all that helpful. It is all flawed, in that it relies heavily on the definition of a miss and recollection bias. The many studies by Perry and colleagues probably provide us with the most useful data on misdiagnosis. Although the CT or LP alone may be imperfect, when you consider the full workup by the physician, there were essentially no misses in any of their very large prospective cohorts.
If the LP is imperfect, should I just order a CT angiogram?
Although multiple guidelines have suggested that this approach is acceptable, I don’t think that routine use is supported by the evidence. (Meurer 2016; Godwin 2019) The risk of SAH after a negative plain CT head is just so low that it is unlikely that any test will help, and the CT angiogram has its own problems. Although it is very sensitive for the aneurysms that lead to SAH, it does not tell us if the aneurysm bled. That is a huge problem, as aneurysms are incredibly common (maybe as high as 7%, but probably closer to 2%) in asymptomatic patients, and most don’t bleed. (Li 2013; Taylor 2016) However, after these aneurysms are discovered, surgeons often feel compelled to treat them, and, unsurprisingly, invasive brain surgery has downsides. Surgery seems particularly high risk, with a 6% rate of aneurysm rupture during surgery, another 4% having intracerebral hemorrhage, 11% suffering an ischemic stroke, and 2% dying. (Wiebers 2003) However, even endovascular management is risky, with a 2% rate of hemorrhage and 5% rate of ischemic stroke (although those numbers are from before 2003). (Wiebers 2003) Based on a review of the literature for their test threshold calculation, Taylor and colleagues estimate the rate of death from surgery for an asymptomatic aneurysm at 2.5% and long term morbidity at 9.2%. (Taylor 2016)
Clearly, we can do tremendous harm to our patients by identifying incidental aneurysms. I think these numbers clearly suggest that CT angio should not be used routinely as a replacement for the lumbar puncture. There is probably a role for carefully selected patients. Personally, I only use it to help guide care after an indeterminate or traumatic lumbar puncture. If there is no aneurysm, I can ignore the blood in the CSF.
So when should I actually perform an LP? The test threshold
The test threshold is an incredibly important concept in medicine. The test threshold attempts to mathematically assess both the risks of missing the condition and the risks of the test itself to determine a pretest probability below which we should not be testing because the test will actually do more harm than good. This is best known in the context of PE, where we know that if a patient has less than a 2% chance of having a PE, we will actually cause the patient harm if we decide to send the DDimer. (I have also previously discussed the related treatment threshold in the context of STEMI.) Luckily for us, multiple authors have attempted to calculate a test threshold for lumbar puncture in the assessment of subarachnoid hemorrhage.
Carpenter and colleagues (2016) calculate that there is a very narrow range in which the benefits of lumbar puncture might outweigh the harms. When using xanthochromia, they calculate that the patient needs a pre-lumbar puncture probability of SAH between 2 and 7% to make LP reasonable. If relying on CSF red cell count, the range is only 2-4%. Below that number, no further testing should be done. Above that number, CT angiogram is their suggested test. These are the post-CT probabilities, which are clearly much higher than the miss rate of CT discussed above. They calculate that you would need a pre-CT probability of SAH of more than 70% to justify lumbar puncture if the CT was done within 6 hours, and more than 20% if the CT was done after 6 hours. (Remember that the prevalence of SAH in emergency department patients with acute onset headaches is about 7%, and it is even lower if the patient presents after 6 hours.)
Another group carried out a similar series of calculations to determine the test threshold for LP in the evaluation of SAH after a negative noncontrast head CT in neurologically normal patients. (Taylor 2016) They assumed a 100% sensitivity of lumbar puncture for SAH, which based on the above is likely incorrect, so their final number is probably too low (although there are lots of assumptions in these calculations that could push the final number in either direction). They come up with a test threshold of 4.3%. They perform a sensitivity analysis, and determine a range of possible test thresholds from 1.9% to 15.6%, with the variability primarily based on uncertainty about the probability of death from a missed SAH.
Whatever the actual number, these numbers are all striking in that they are an order of magnitude higher than a patient’s risk after a negative CT within 6 hours, and are even significantly higher than a patient’s risk after a negative CT after 6 hours.
The Taylor paper suggests that carefully selected patients with a very high (>20%) pretest probability of SAH who present late (more than 2 days after symptoms onset) may benefit from lumbar puncture, but that for the vast majority of patients the harms of lumbar puncture outweigh any potential benefit. (Taylor 2016)
Summary
A plain CT head misses very few cases of subarachnoid hemorrhage, even if that CT was done more than 6 hours after symptom onset. The miss rate of a CT done within 6 hours is close to 2 in 1,000. Even if the CT was done after 6 hours, post-test probability is less than 1%. Considering the harms of lumbar puncture, it is clear that the test should not be performed routinely if subarachnoid hemorrhage is the only concern. Of course, there is a much broader differential for a patient with a severe headache, so lumbar puncture will remain a part of the work-up for many patients, based on physician judgement, and hopefully involving patients as part of shared decision making.

First10EM Evidence Based Medicine Resources
Evidence based medicine is easy
Evidence based medicine resources
Other Subarachnoid Hemorrhage FOAMed
Let’s talk about subarachnoid haemorrhage – St Emlyn’s
EMCases Episode 14 Part 1: Migraine Headache and Subarachnoid Hemorrhage
EM Lit of Note: Is the 6-Hour CT for SAH Debate Over?
REBEL EM: Does a Normal Head CT Within 6 Hours of Onset of Headache Rule Out SAH? and Validation of the Ottawa Subarachnoid Hemorrhage Rule in Patients With Acute Headache and The Ottawa SAH Clinical Decision Rule and Xanthochromia Detection: Visual Inspection vs. Spectrophotometry
SGEM#201: It’s In The Way That You Use It – Ottawa Sah Tool
SGEM#283: Can You Be Absolutely Right In Diagnosing A Sah Using A Clinical Decision Instrument?
References
Backes D, Rinkel GJ, Kemperman H, Linn FH, Vergouwen MD. Time-dependent test characteristics of head computed tomography in patients suspected of nontraumatic subarachnoid hemorrhage. Stroke. 2012;43(8):2115-2119. doi:10.1161/STROKEAHA.112.658880 PMID: 22821609
Blok KM, Rinkel GJ, Majoie CB, et al. CT within 6 hours of headache onset to rule out subarachnoid hemorrhage in nonacademic hospitals. Neurology. 2015;84(19):1927-1932. doi:10.1212/WNL.0000000000001562 PMID: 25862794
Carpenter CR, Hussain AM, Ward MJ, et al. Spontaneous Subarachnoid Hemorrhage: A Systematic Review and Meta-analysis Describing the Diagnostic Accuracy of History, Physical Examination, Imaging, and Lumbar Puncture With an Exploration of Test Thresholds. Acad Emerg Med. 2016;23(9):963-1003. doi:10.1111/acem.12984 PMID: 27306497
Carstairs SD, Tanen DA, Duncan TD, et al. Computed tomographic angiography for the evaluation of aneurysmal subarachnoid hemorrhage. Acad Emerg Med. 2006;13(5):486-492. doi:10.1197/j.aem.2005.12.010 PMID: 16551778
Chu K, Hann A, Greenslade J, Williams J, Brown A. Spectrophotometry or visual inspection to most reliably detect xanthochromia in subarachnoid hemorrhage: systematic review. Annals of emergency medicine. 64(3):256-264.e5. 2014. PMID: 24635988
Chu KH, Keijzers G, Furyk JS, et al. Applying the Ottawa subarachnoid haemorrhage rule on a cohort of emergency department patients with headache. Eur J Emerg Med. 2018;25(6):e29-e32. doi:10.1097/MEJ.0000000000000523 PMID: 29215380
Davenport R. Acute headache in the emergency department. J Neurol Neurosurg Psychiatry. 2002;72 Suppl 2(Suppl 2):ii33-ii37. doi:10.1136/jnnp.72.suppl_2.ii33
Dubosh NM, Bellolio MF, Rabinstein AA, Edlow JA. Sensitivity of Early Brain Computed Tomography to Exclude Aneurysmal Subarachnoid Hemorrhage: A Systematic Review and Meta-Analysis. Stroke. 2016;47(3):750-755. doi:10.1161/STROKEAHA.115.011386 PMID: 26797666
Godwin SA, Cherkas DS, et al. Clinical Policy: Critical Issues in the Evaluation and Management of Adult Patients Presenting to the Emergency Department With Acute Headache. Ann Emerg Med. 2019;74(4):e41-e74.
Goldstein J, Camargo C, Pelletier A, Edlow J. Headache in United States Emergency Departments Cephalalgia. 2016; 26(6):684-690.
Gorchynski J, Oman J, Newton T. Interpretation of traumatic lumbar punctures in the setting of possible subarachnoid hemorrhage: who can be safely discharged?. Cal J Emerg Med. 2007;8(1):3-7. PMID: 20440386
Kowalski RG, Claassen J, Kreiter KT, et al. Initial misdiagnosis and outcome after subarachnoid hemorrhage. JAMA. 2004;291(7):866-869. doi:10.1001/jama.291.7.866 PMID: 14970066
Li MH, Chen SW, Li YD, et al. Prevalence of unruptured cerebral aneurysms in Chinese adults aged 35 to 75 years: a cross-sectional study. Ann Intern Med. 2013;159(8):514-521. doi:10.7326/0003-4819-159-8-201310150-00004 PMID: 24126645
Mark DG, Sonne DC, Jun P. False negative interpretations of cranial computed tomography in aneurysmal subarachnoid hemorrhage. Academic emergency medicine : official journal of the Society for Academic Emergency Medicine. 2016. PMID: 26918885
Menke J, Larsen J, Kallenberg K. Diagnosing cerebral aneurysms by computed tomographic angiography: meta-analysis. Ann Neurol. 2011;69(4):646-654. doi:10.1002/ana.22270 PMID: 21391230
Meurer WJ, Walsh B, Vilke GM, Coyne CJ. Clinical Guidelines for the Emergency Department Evaluation of Subarachnoid Hemorrhage. J Emerg Med. 2016;50(4):696-701.
Nath S, Koziarz A, Badhiwala JH, et al. Atraumatic versus conventional lumbar puncture needles: a systematic review and meta-analysis. Lancet. 2018;391(10126):1197-1204. doi:10.1016/S0140-6736(17)32451-0 PMID: 29223694
Perry JJ, Stiell IG, Sivilotti ML, et al. High risk clinical characteristics for subarachnoid haemorrhage in patients with acute headache: prospective cohort study. BMJ. 2010;341:c5204. Published 2010 Oct 28. doi:10.1136/bmj.c5204 PMID: 21030443
Perry JJ, Stiell IG, Sivilotti ML, et al. Sensitivity of computed tomography performed within six hours of onset of headache for diagnosis of subarachnoid haemorrhage: prospective cohort study. BMJ. 2011;343:d4277. Published 2011 Jul 18. doi:10.1136/bmj.d4277 PMID: 21768192
Perry JJ, Stiell IG, Sivilotti ML, et al. Clinical decision rules to rule out subarachnoid hemorrhage for acute headache. JAMA. 2013;310(12):1248-1255. doi:10.1001/jama.2013.278018 PMID: 24065011
Perry JJ, Alyahya B, Sivilotti ML, et al. Differentiation between traumatic tap and aneurysmal subarachnoid hemorrhage: prospective cohort study. BMJ. 2015;350:h568. Published 2015 Feb 18. doi:10.1136/bmj.h568 PMID: 25694274
Perry JJ, Sivilotti MLA, Sutherland J, et al. Validation of the Ottawa Subarachnoid Hemorrhage Rule in patients with acute headache [published correction appears in CMAJ. 2018 Feb 12;190(6):E173]. CMAJ. 2017;189(45):E1379-E1385. doi:10.1503/cmaj.170072 PMID: 29133539
Perry JJ, Sivilotti MLA, Émond M, et al. Prospective Implementation of the Ottawa Subarachnoid Hemorrhage Rule and 6-Hour Computed Tomography Rule. Stroke. 2020;51(2):424-430. doi:10.1161/STROKEAHA.119.026969 PMID: 31805846
Rinkel GJ, Djibuti M, Algra A, van Gijn J. Prevalence and risk of rupture of intracranial aneurysms: a systematic review. Stroke. 1998;29(1):251-256. doi:10.1161/01.str.29.1.251 PMID: 9445359
Sayer D, Bloom B, Fernando K, et al. An Observational Study of 2,248 Patients Presenting With Headache, Suggestive of Subarachnoid Hemorrhage, Who Received Lumbar Punctures Following Normal Computed Tomography of the Head. Acad Emerg Med. 2015;22(11):1267-1273. doi:10.1111/acem.12811 PMID: 26480290
Seupaul RA, Somerville GG, Viscusi C, Shepard AJ, Hauter WE. Prevalence of postdural puncture headache after ED performed lumbar puncture. Am J Emerg Med. 2005;23(7):913-915.
Taylor RA, Singh Gill H, Marcolini EG, Meyers HP, Faust JS, Newman DH. Determination of a Testing Threshold for Lumbar Puncture in the Diagnosis of Subarachnoid Hemorrhage after a Negative Head Computed Tomography: A Decision Analysis. Acad Emerg Med. 2016;23(10):1119-1127. doi:10.1111/acem.13042 PMID: 27378053
Vermeulen MJ, Schull MJ. Missed diagnosis of subarachnoid hemorrhage in the emergency department. Stroke. 2007;38(4):1216-1221. doi:10.1161/01.STR.0000259661.05525.9a PMID: 17322078
Wiebers DO, Whisnant JP, Huston J 3rd, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003;362(9378):103-110. doi:10.1016/s0140-6736(03)13860-3 PMID: 12867109
Youssef NA, Gordon AJ, Moon TH, et al. Emergency department patient knowledge, opinions, and risk tolerance regarding computed tomography scan radiation. J Emerg Med. 2014;46(2):208-214. doi:10.1016/j.jemermed.2013.07.016 PMID: 24063878
Morgenstern, J. Subarachnoid Hemorrhage: What is the role of LP?, First10EM, September 21, 2020. Available at:
https://doi.org/10.51684/FIRS.42400




14 thoughts on “Subarachnoid Hemorrhage: What is the role of LP?”
“I have always wondered, why not just directly measure the chemicals that make the fluid yellow? I mean, every lab has the capacity to measure bilirubin. Why don’t we just send CSF for bilirubin? ” Great Question and Truly Translational…(and one that I had myself at one time) It ties together multiple topics I often lecture on…additionally, your question applies not only in the context you present, but also in that of premature neonates with IVHs secondary to germinal matrix hemorrhage. SHORT ANSWER: It is a question of both timing and confounding variables that can also potentially increase CSF bilirubin. Clinical Relevance: CSF bili is not always a reliable or time sensitive standalone modality… we can often make a rapid definitive dx and initiate tx without it… it wouldn’t necessarily alter the patient’s patient projected clinical course in a value added fashion… (additional NB: It can also vary somewhat by analysis suite, so with questions like these, I always recommend contacting your lab director for an often truly in depth discussion of additional variables that may not be readily apparent to bedside clinicians.)
Thanks for the thorough answer.
I wonder if any of those responses are different for xanthromchromia? Have we chosen xanthrochromia for historical reasons, or has someone actually thought this through and decided it is better than measuring bili directly?
Justin, this is an excellent post, and highlights some of the questions that we have all struggled with as we learn and re-learn the approach to diagnosing SAH in the ED. Your conclusion seems very definitive in “Considering the harms of lumbar puncture, it is clear that the test should not be performed routinely if subarachnoid hemorrhage is the only concern”.
I worry about abandoning the LP altoghether for SAH diagnosis given the lack of robust evidence. I wonder if there is still a role in a patient that you percieve as high risk based on presentation (thunderclap headach, worst, loss of conciousness) EVEN with a negative CT (especially after 6 or even 12 hours).
I would at least advocate for a role in shared decision making — of course, exactly how to frame this shared decision become the issue…
Thanks again for this review!
Thanks Leeor
I struggle a bit with the terminology. I don’t think it should be “routine”. However, I end up doing an LP for SAH every couple months at least, so it also isn’t contraindicated. (And these LPs are always in the context of shared decision making.) However, in the context of the test threshold calculations, I do struggle to figure out exactly which patients need an LP, and I think we have probably been somewhat overdoing them to date.
SAH
One of my favourite clinical topics excellently delivered by my favourite blog!
I do a lecture on this with the same conclusions – we need to consider the post-test probability logically and therefore know about our (along with the patients ) “acceptable miss rate”. I guess there might be an argument that Klines 2% threshold for PE and ACEPs 2% ACS threshold may not apply to SAH as it is a higher risk of being more devastating if missed (though that does not mean we shouldn’t have the “acceptable miss rate “ conversation!!!)
I have a few minor comments and one bigger one:
The minor ones
1: prevalence of sah: around 10% in Sweden , ED (in Denmark and I think back then in Sweden our EDs were filtered in a different way = not open to everyone , but needs to see a GP who does the “filtering “. That might explain the higher acuity )
2: The CT angio argument : I think Dr Jerome Hoffman argued for the use of CT and then angio if it was negative (following the patient to the radiologist, so they wouldn’t have to go twice ). I hear this argument at my lectures and I think also from among other Dr Jonathan Edlow (https://pubmed.ncbi.nlm.nih.gov/28601276/ ) and Orr et al (https://www.amazon.com/Emergency-Headache-Management-Serena-Orr/dp/1107177200) – the argument from the latter are that they “think” (professional opinion, no reference) that 10-20% with TCH have a serious condition that may only be found out with CT angio (I.e RCVS, the minority of CVST presenting with TCH, cervical artery disssction etc). I would argue that the pretest probability is so low that the risk of false positive probably outweighs the benefit of waiting (I.e. RCVS come back and only 5% have ischemic events that from my knowledge are not really preventable with current medical treatment … so one my argue , why try to find them ?)
My major comment is also one of my take home points
– I see no one doing studies on one of the most important topics : how we asses the pretest probability through the history taking . The way we take this history (not only in headache patients ) is monumentally important for assessing the pretest probability . If we do not lead with an open question and pick out the criteria for TCH from the uninterrupted patient story telling , we are very prone to “priming “ the patients answer (I.e did your headache come suddenly is a “yes”-“no” answer , they are in the Ed , are scared and maybe even embarrassed/ want to “get all the tests” etc and therefore in any headache err on the “yes” side to that question more than the “no” side.
As fuller said in his excellent “neurology made easy”
“Remember that a spontaneously reported symptom is much more significant than one obtained on direct questioning. For example, patients rarely volunteer that their headaches get worse on coughing or sneezing, and when they do it suggests raised intracranial pressure. In contrast, many patients with tension-type headaches and migraine will say their headaches get worse in these situations if directly asked about them”
In other words the “test” that is our history taking (which we do not know how went down in these studies by perry et al) in the monosymptomatic headache patients , is a thing that we should be talking much more about (I think we do a poor job selecting the right patients). The risk of not doing that will (and do) risk framing bias, premature closure and ultimately overdiagnosis (often entirely missing what the patients “problem” – not chief complaint – was)
That’s my additions to an as always amazing post!
Thanks for the most in depth comment the website has ever received – totally agree
Thanks for this great summary. For patients presenting late I wonder if the best strategy for late-presenting patients with normal CT is to perform a CTA initially. If this shows an aneurysm an LP can be performed to determine if it has bled. Have you found any research looking at this approach?
I worry about the number of false positives in this strategy. CTA finds a lots of incidental aneurysms, and finding these can cause a lot of harm. I think the best answer at this point is that we just don’t know. We need better research helping us pick out who is at highest risk among these late presenters. For the most part, because most patients with SAH present early, I think plain CT will be enough, but you will have to take it on a case by case basis, and decide between LP and CTA in those patients who you think are very high risk.
My question is why are they going after asymptomatic aneurysm given the high morbidity. The data cited is fairly old, I would if there is further advancement on risk stratifying which aneurysm needs intervention and which one doesn’t (not binary but rather as a spectrum). I think thats the key bugaboo here, there seems to be much room to be made in the better understanding and decreasing the harm of incidental aneurysms, if we can do this, CTA appears like the best option. Further I might be simple, but why do we miss leaking SAH on CTA anyways? Not enough slices?
I think improvement of imaging and analysis of imaging results is the way