
Time for another semi-regular round-up of the top emergency medicine and critical care articles I have encountered over the last few months. This time we will tackle anti-epileptics, anti-emetics, the word “quiet”, and a whole bunch more…
Our second line agents for status epilepticus all suck
ESETT: Kapur J, Elm J, Chamberlain JM, et al. Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus. The New England journal of medicine. 2019; 381(22):2103-2113. PMID: 31774955
This is the third big RCT this year comparing levetiracetam to other options as the second line treatment of status epilepticus, and once again (despite tremendous hype) it wasn’t any better. They randomized 400 episodes of status epilepticus to receive either fosphenytoin (20mg/kg PE), valproate (40 mg/kg), or levetiracetam (60 mg/kg) as the second line agent for seizing patients. Unfortunately, not all patients were actually seizing, 27% failed to meet their eligibility criteria, and patients had already been seizing for an hour before enrollment. Furthermore, it isn’t clear to me that the doses used are equivalent, so the test might not have been that fair from the outset. However, in the end, the results for each group were identical. There has never been a reason to adopt the newer (and for a long time significantly more expensive) levetiracetam. After 3 negative trials, I will stick with our older agents, but honestly – these drugs all sort of suck, and I tend to use propofol as my second line agent.
Bottom line: There was no difference between levetiracetam, valproate, and fosphenytoin as the second line agent in status epilepticus.
Hearts have memory?
Peck D, Al-Kaisey A. Cardiac memory: an under-recognised cause of deep T wave inversion in a patient presenting with chest pain. BMJ case reports. 2018; 2018:. PMID: 30061136
Gautschi O, Naegeli B. Cardiac memory mimicking myocardial ischaemia. Journal of the Royal Society of Medicine. 2003; 96(3):131-2. PMID: 12612116
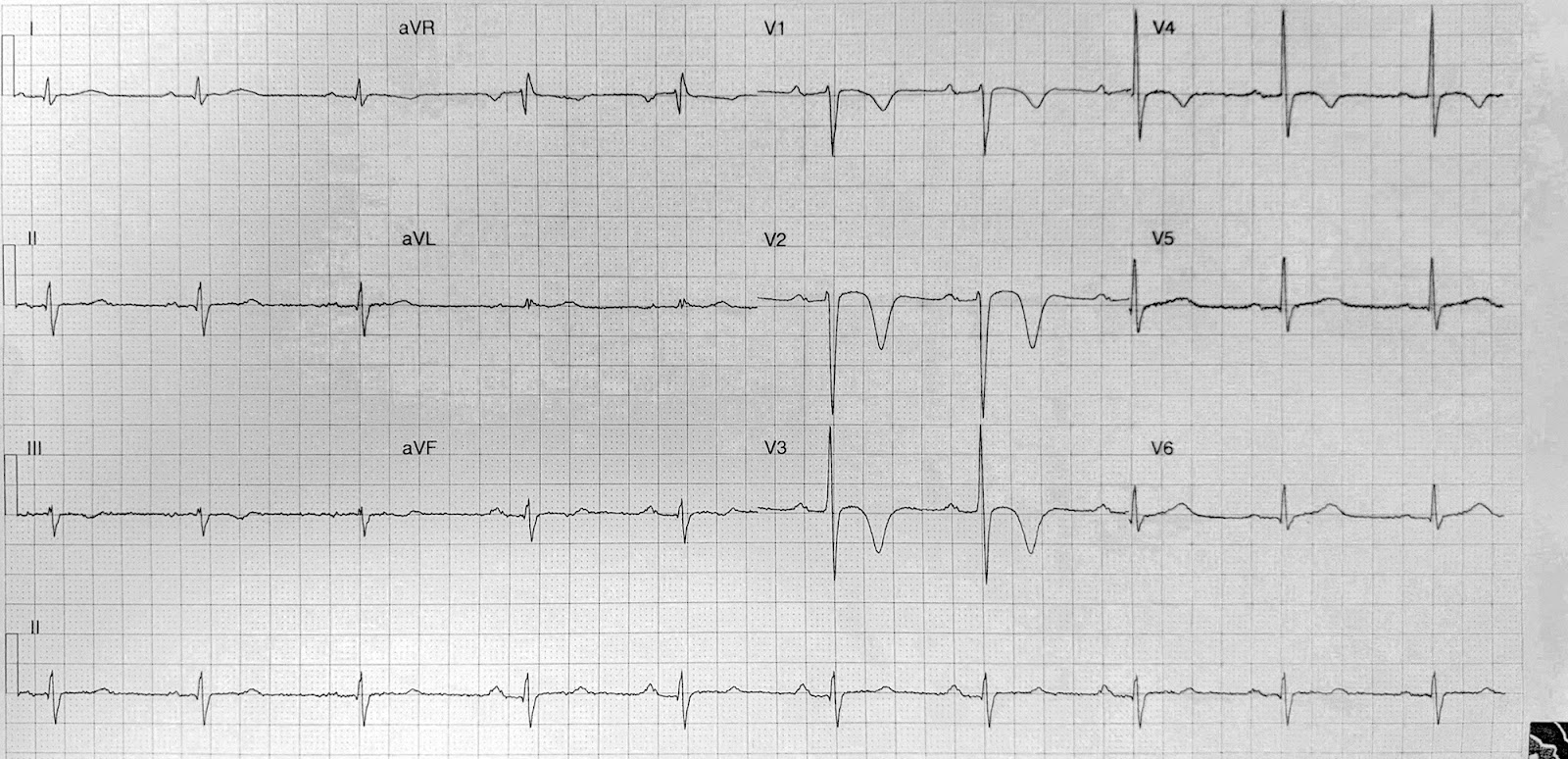
I found these papers because of an interesting case. A previously healthy man was brought in to the trauma team after being injured by a cow (perhaps the most common trauma activation in New Zealand). The injuries seemed to be entirely centered around this hip and lower abdomen. His vital signs were always in the normal range, and he looked quite well. However, a “routine” ECG was printed off in the resus bay, and as you can see below, it showed deep anterior T waves that reminded me a lot of Wellen’s syndrome. However, it couldn’t have been Wellen’s, because he had absolutely no symptoms, despite my persistent questioning and insistence that he must. There was never any chest pain, shortness of breath, diaphoresis, dizziness, nausea, vomiting, arm pain, neck pain, back pain, or anything at all that I could call an ACS equivalent at any time before or after the trauma.
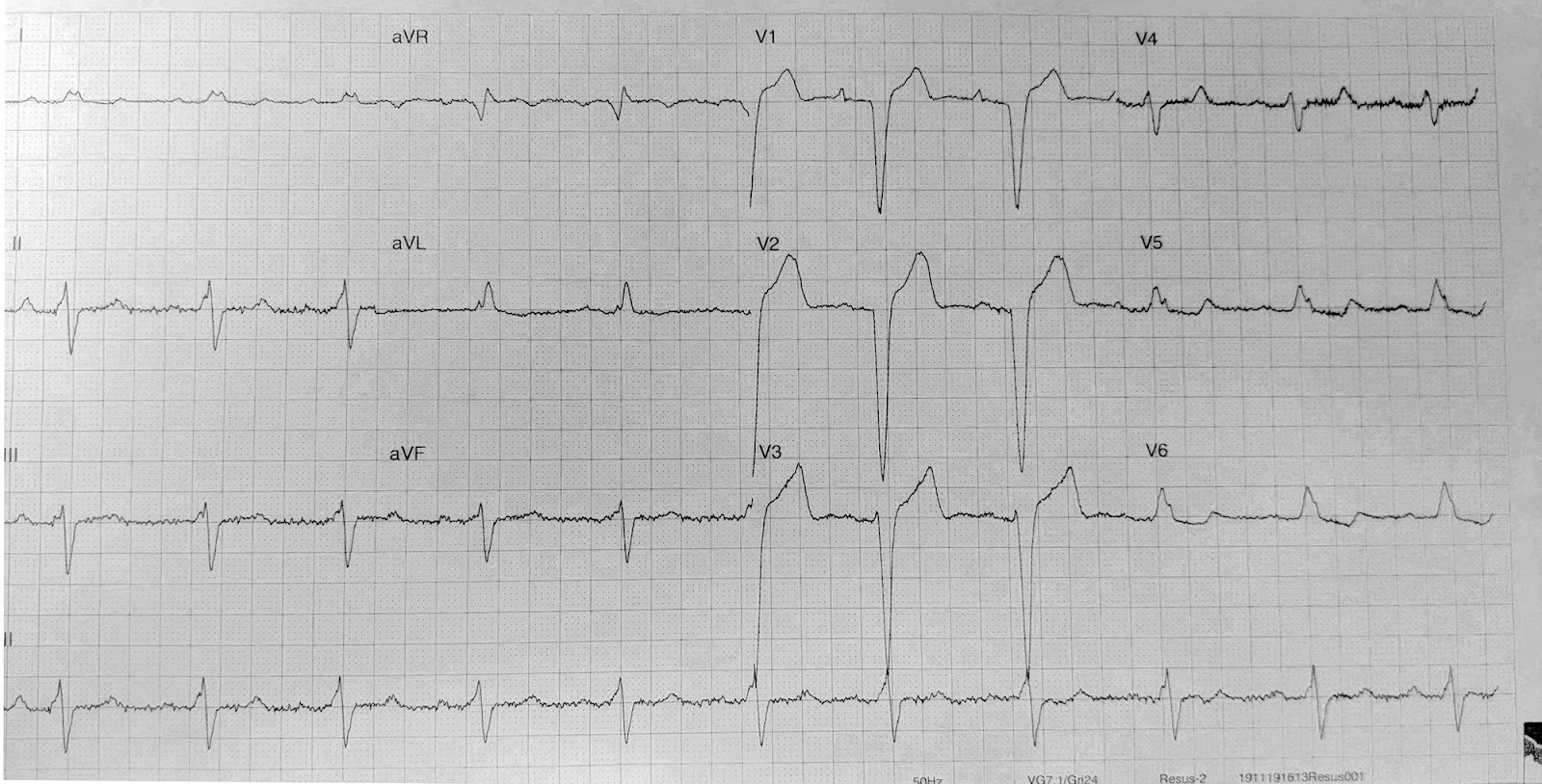
When we repeated the ECG, it had changed. Now there was a left bundle branch block, and although there is ST elevation in the anterior leads, it is proportional to the large QRS complexes, and I think it is clearly a non-ischemic ECG. We did a bedside echo, that was essentially normal. He had 3 normal troponins in the ED. We added the thorax to his trauma CT scan because of the ECG, but it was completely normal. We chatted with the medicine team and the cardiologist on call, and they were concerned, but weren’t sure about the diagnosis. Ultimately, we admitted him to the ICU for monitoring and he was fine.
As you can see from the rhythm strip below, he would just flip back and forth between the two different complexes. (Ignore the size of the ST elevation – the rhythm strip distorts it. The complexes were actually identical to those in the 12 lead ECGs above).
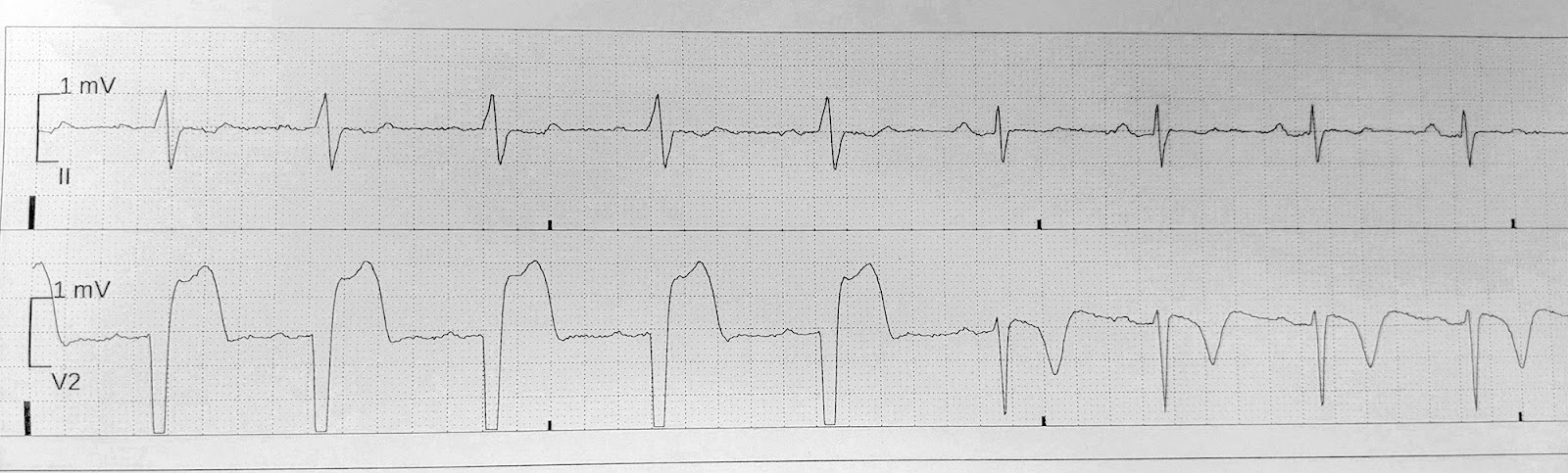
I was baffled, so I turned to Twitter for some help. It was Sam Ghali (@EM_RESUS) that ultimately came up with what I believe to be the right diagnosis: cardiac memory. I had never heard of “cardiac memory” before. (It is also sometimes called “Chatterjee phenomenon”). Apparently, after being in a ventricular rhythm, the T wave “remembers” or tends to persist along the same vector. The result is that you can get deep T wave inversions just like I saw. This is commonly seen after temporary pace-makers and in the EP lab, but it can also happen after an intermittent left bundle branch block, like we saw in my case. It is generally considered benign. That being said, if I see a similar ECG again in the future, I will definitely be discussing it with someone before just writing it off as cardiac memory.
Peripheral pressor update
Pancaro C, Shah N, Pasma W, et al. Risk of Major Complications After Perioperative Norepinephrine Infusion Through Peripheral Intravenous Lines in a Multicenter Study. Anesthesia and analgesia. 2019; PMID: 31569163
I’ve covered this topic before. This chart review looks at 14,385 patients that received peripheral norepinephrine during surgery at 2 hospitals in the Netherlands. Only 5 patients (0.035%) had an extravasation event and none had significant skin injuries. This is the largest study to date looking at adverse events with peripheral vasopressors. However, largest doesn’t necessarily mean best. Previous estimates suggest a 3-4% risk of extravasation (although with a similarly low rate of actual skin injuries). The very low incidence seen here might be because events were overlooked in the chart review, or simply not reported. It is also possible that these OR patients are just different than our ED patients.
Bottom line: I think we are likely to see much higher rates of extravasation in the ED, but because true harms are rare, the overall message is still correct: if monitored carefully, it is perfectly reasonable to give norepinephrine through a well functioning peripheral IV.
His arm is bent!! Are you seriously just going to leave it like that!?!?!
Crawford SN, Lee LS, Izuka BH. Closed treatment of overriding distal radial fractures without reduction in children. The Journal of bone and joint surgery. American volume. 2012; 94(3):246-52. PMID: 22298057
This is a retrospective case series of patients from the office of a single orthopedic surgeon, so the evidence level might not be what we are used to, but I think it is still interesting enough to look at. He took 51 children aged 10 years and younger with overriding fractures of the distal radial metaphysis, with or without an ulnar fracture, and managed them all without reduction. Overriding meant 100% dorsal translation and shortening of the distal segment. Neurovascular injuries and growth plate injuries were important exclusions. Despite significant deformity, only seven of these children had reduction attempts prior to being sent to his clinic, and obviously all of those attempts failed. Treatment was without reduction, although he did perform “gentle correction of angulation” when applying the cast, with a goal of less than 10 degrees of angulation. (These “gentle manipulations” always concern me, and in my mind generally need sedation or a nerve block anyway. If that is the case, why not just perform the full reduction?) There was an average of 5 mm of shortening and 4 degrees of angulation at the time of casting, and many of the patients had an obvious dinner fork deformity when they were placed in the cast. When the case was removed, none of the patients had a clinical deformity, all had full range of motion and good grip strength, and all had returned to their normal activities. All patients were satisfied with the treatment. The images in the paper are pretty dramatic. Obviously, this is a small study with a high degree of bias. He does cite 2 other papers that report similar results, but I don’t think I am changing my practice overall. However, I think these images are nice to see, because we often become rather perfectionist when performing reductions. It is good to know that even significant deformities can have very good outcomes in children. It might save the occasional child an repeat sedation for a second (or third) reduction attempt.


Bottom line: Pediatric fractures undergo a tremendous amount of re-modeling. We might be overdoing our reductions somewhat, especially now that sedations are relatively easy to perform in most EDs.
Using a facemask to blind children (that sounds sort of bad)
Tsze DS, Woodward HA. The “Facemask Blinder”: A Technique for Optimizing Anxiolysis in Children Undergoing Facial Laceration Repair. Pediatric emergency care. 2019; 35(7):e124-e126. PMID: 27941503
If you are going to send me home from the emergency department with a bent arm, you better make sure I can’t see it. This paper has a quick clinical tip that I found interesting. They use the standard surgical face mask, and tie it so it is pointing straight out from the face to act as a blinder, so that children can’t see what you are doing. You can place the mask either above or below the eyes. They suggest cutting off the second set of ties, so they don’t get in the way. Of course, some kids find it even more anxiety provoking not to be able to see what is going on, so there isn’t a one size fits all strategy. For more tips and tricks on making hospitals less scary, see this post.


Are antiemetics useless?
Meek R, Mee MJ, Egerton-Warburton D, et al. Randomized Placebo-controlled Trial of Droperidol and Ondansetron for Adult Emergency Department Patients With Nausea. Academic emergency medicine. 2019; 26(8):867-877. PMID: 30368981
This is an RCT that compared both ondansetron and droperidol to placebo. The headline news was that neither of our favoured agents beat placebo when nausea was measured at 30 minutes. However, if you look a little closer, the droperidol group required less rescue medication and had a higher number of patients who said they felt better. There have been a number of studies claiming that our anti-emetics have no effect. We almost certainly overuse these agents, but I think the truth is probably more complicated. Personally, I find nausea and vomiting worse than pain, and would want it treated if I showed up at an emergency department.
Bottom line: Our anti-emetics probably aren’t as effective as we like to think, but they are probably better than this trial makes them seem.
Martial arts technique for control of severe external bleeding
Slevin JP, Harrison C, Da Silva E, White NJ. Martial arts technique for control of severe external bleeding. Emergency medicine journal : EMJ. 2019; 36(3):154-158. PMID: 30612092
I don’t know when this technique will ever be relevant, especially because I keep tourniquets in my medical bag, work locker, home, and car (what can I say – they are cheap on amazon.) Using a trained Brazilian jiu-jitsu black belt, they used a modified knee mount hold to apply pressure at three different locations (shoulder, groin, and abdomen), and then used Doppler ultrasound measurements as a surrogate for adequate arterial compression. The brachial and femoral artery compression resulted in pretty significant drops in flow, but the trans-abdominal aorta compression was less impressive. Of course, this is a single center study with healthy volunteers using a surrogate outcome, but if you happened upon a trauma scene, and for some reason don’t have a tourniquet available, I suppose this could represent a life saving maneuver while waiting for EMS. I guess we should compare it to the standard movie trope of using your belt.

Could an ED-ICU combination unit save lives?
Gunnerson KJ, Bassin BS, Havey RA, et al. Association of an Emergency Department-Based Intensive Care Unit With Survival and Inpatient Intensive Care Unit Admissions. JAMA network open. 2019; 2(7):e197584. PMID: 31339545 [free full text]
Although I will probably never work in a place that has one, I find the concept of an ED-ICU both intriguing and concerning. This is a before and after look at the introduction of an ED-ICU in Michigan. Based on raw numbers, overall mortality in the ED was exactly the same before and after the unit opened. However, patients were getting older and sicker with time, so when they did an adjusted analysis, they found that there was a lower mortality for ED patients after the unit was opened. The inherent flaws in before and after studies, and the fact that the difference only shows up in the adjusted data, mean that we shouldn’t be rushing to open ED-ICUs in every hospital. However, it might be beneficial to consider the differences between ED and ICU settings, and what processes we might adopt to improve outcomes for our patients in the ED.
Bottom line: Don’t redesign your hospital yet, but conversations between ICU and ED to ensure processes are in place so that patients get the best possible care no matter where they are physically situated sound like a good idea.
I am sure everyone working over the holidays this year has noticed how quiet it has been
Brookfield CR, Phillips PPJ, Shorten RJ. Q fever-the superstition of avoiding the word “quiet” as a coping mechanism: randomised controlled non-inferiority trial. BMJ (Clinical research ed.). 2019; 367:l6446. PMID: 31852676 [free full text]
Some people have coined the concept of science based medicine as an improvement on evidence based medicine. The idea is that you need to consider the scientific plausibility of a concept before simple doing studies. You can consider homeopathy in the context of evidence based medicine, because there are many studies, and therefore lots of evidence. Science based medicine tells us that is silly. There is no possibility that homeopathy works. Those studies should never have been done. If a study is positive, it is clearly because of random chance or bias, because homeopathy has no basis in reality.
Saying quiet cannot possibly impact the number of sick patients in the community. It cannot possibly make your shift busier (although it might make you feel busier subjectively, if you are superstitious). Thus, science based medicine would probably tell us that this fun randomized control trial from the BMJ Christmas edition should never have been performed. For 61 consecutive days, this team was randomized to either start the day by saying “today will be a quiet day” or to refrain from saying the word “quiet”. They then tracked the total amount of work that was done that day (this was a medical lab, and so the tasks can be measured somewhat objectively). Before starting, they determined that 10 extra tasks per team member would make a day noticeably busier, so that was their margin of non-inferiority. During their 61 day trial, there were 2 full moons and a summer solstice, but no Friday the 13ths. The mean number of clinical events was 139 on control days and 145 on days when they said “quiet”, which was non-inferior according to their definition. There was in imbalance in randomization between weekends and weekdays. When this was adjusted for, the exact same number of tasks were performed, whether or not quiet was said. They do note that they did not control for other confounding factors, such as the “presence of black cats, cracked mirrors, or lone magpies.” “Areas for further research include whether horse shoes placed outside patient isolation rooms can prevent the transmission of resistant organisms, whether a rabbit’s foot in theatre can reduce surgical site infections, and whether being touched by a royal can cure tuberculosis.”
Bottom line: Obviously saying quiet cannot possibly impact how busy a hospital is. Don’t @ me.
Cheesy Joke of the Month
What do you call a bear with no teeth?
A gummy bear
Morgenstern, J. Research Roundup (January 2020), First10EM, January 20, 2020. Available at:
https://doi.org/10.51684/FIRS.10450


