
Morgenstern, J. Research Roundup (August 2021), First10EM, August 16, 2021. Available at:
https://doi.org/10.51684/FIRS.83756
My morning ritual of reading articles over coffee has transformed somewhat, such that there is a lot more playing with an infant, and a lot less evidence based medicine. Although the coffee isn’t going anywhere, it is usually cold by the time I have a free moment to get to it. Therefore, these EBM updates are likely to be a lot less frequent over the next couple of years. However, I still have a massive backlog in my “to be read” folder, and the journals won’t stop pumping out (mostly poor quality) studies, so I will attempt to keep hammering away…
Antibiotics won’t work for your virus, but take these antibiotics in a couple days anyway
Mas-Dalmau G, Villanueva López C, et al. Delayed Antibiotic Prescription for Children With Respiratory Infections: A Randomized Trial. Pediatrics. 2021 Mar;147(3):e20201323. doi: 10.1542/peds.2020-1323. Epub 2021 Feb 11. PMID: 33574163
This is another RCT that demonstrates the harms of delayed antibiotic prescriptions. It is a multicentre RCT of pediatric patients from primary care pediatrics offices. They randomized 436 patients with respiratory tract infections (mostly pharyngitis and otitis media) in whom the physician had a reasonable doubt about the value of antibiotics to one of three groups: immediate antibiotics, delayed antibiotics, or no antibiotics. The prescription strategy worked, with 96% of the immediate group taking antibiotics, as compared to 25% of the delayed antibiotic group, and 12% of the no antibiotic group (all statistically significant). However, that was the only difference. There was no change in their primary outcome, or any of the very many secondary outcomes looking at symptoms between the groups. There were no differences in complications, unscheduled visits, or satisfaction. The only difference was that antibiotics increased GI side effects. We should expect significant bias towards the antibiotic groups in this unblinded trial, so the results are probably even worse than they seem. Therefore, as compared to appropriate medical care (not prescribing antibiotics when they are not indicated), a delayed prescription leads to a significant increase in antibiotic use without clinical benefit. (More details can be found here.)
Bottom line: Delayed antibiotics don’t make sense. Antibiotics don’t magically start treating viruses just because you wait 2 days.
More Peds ID: Tympanostomy tubes don’t work
Hoberman A, Preciado D, Paradise JL, et al. Tympanostomy Tubes or Medical Management for Recurrent Acute Otitis Media. N Engl J Med. 2021 May 13;384(19):1789-1799. doi: 10.1056/NEJMoa2027278. PMID: 33979487
A very common question, when I explain to students and residents that antibiotics are not necessary for otitis media, is: “how will we identify the kids who need tubes?” Despite the fact that this practice is incredibly widespread, the evidence for tympanostomy tubes has always been fairly mixed. This is a multi-center RCT that randomized 250 children, aged 6 to 35 months, with recurrent otitis media, to either surgical or medical management. There was no difference between the groups, with 1.5 recurrent infections in both groups during the 2 year follow up. The secondary outcomes were mixed, with more days of otitis related symptoms in the medical group, but more days of otorrhea in the surgical group. The quality of life numbers were identical. There was more diarrhea in the medical management group, which is not surprising with the use of amoxicillin-clavulanate. However, considering that the antibiotics were almost certainly unnecessary, this harm seems artificial and unnecessary (and wouldn’t be present if I was treating the child). There are a few problems with this trial. Perhaps the biggest is the primary outcome. I thought the ultimate goal of tympanostomy tubes was improved hearing, and not just a reduction in the number of infections, but this trial doesn’t look at hearing at all. There was a lot of crossover, with 10% of the surgical group not having surgery and 30% of the medical group getting surgery, so the groups will naturally look similar. The medical management group was receiving antibiotics for their infections, which complicates things a little, as we really shouldn’t be prescribing antibiotics for acute otitis media.
Bottom line: Ultimately, I don’t think this trial definitively proves that there is no role for tympanostomy tubes, but considering that there was never great evidence for the practice in the first place, it really should curtail the practice. At this point, I would want to see a positive study before I subjected my child to surgery.
Back to BaSICS: Normal saline is just fine
Zampieri FG, Machado FR, et al. Effect of Intravenous Fluid Treatment With a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial. JAMA. 2021 Aug 10. doi: 10.1001/jama.2021.11684. PMID: 34375394 [free full text]
This is a massive trial that I think confirms what we already knew, but might surprise some people. It is a very well done, double blind RCT of almost 11,000 ICU patients comparing balanced IV fluids (Plasma-Lyte-148) to normal saline. There was absolutely no difference in the primary outcome of all cause mortality (26% versus 27%, adjusted HR, 0.97 [95% CI, 0.90-1.05]; P = 0.47). There was also no change in the key secondary outcomes of need for dialysis (1% vs 1%) or kidney injury (27% vs 27%). There was a statistically significant finding in one subgroup: 90 day mortality was a lot higher with balanced fluids in patients with traumatic brain injury (21% versus 31%, p=0.02), but the numbers were relatively small, the confidence intervals wide, and I don’t believe they adjusted their statistics for multiple comparisons. In my mind, the best available science always suggested normal saline was just fine. People got really excited about the SMART and SALT-ED trials, but they were trials with very imperfect methodology and mixed results. Before BaSICS, the highest quality trial we had was SPLIT, and it also showed no harm from normal saline. Of course, there is no compelling reason to choose normal saline, and nothing wrong with a balanced solution. However, some people talk as if hanging a bag of saline is equivalent to putting a gun to the patient’s head, and those people are clearly wrong.
Bottom line: This is the best evidence to date, and there does not appear to be anything harmful about using normal saline as your IV fluid of choice.
Intense oxygen therapy in palliative care: on oxymoron?
Ruangsomboon O, Dorongthom T, Chakorn T et al. High-Flow Nasal Cannula Versus Conventional Oxygen Therapy in Relieving Dyspnea in Emergency Palliative Patients With Do-Not-Intubate Status: A Randomized Crossover Study. Ann Emerg Med. 2020 May;75(5):615-626. doi: 10.1016/j.annemergmed.2019.09.009. PMID: 31864728
Although this is a low quality study (small, single centered, and unblinded), I think it will (and should) be practice changing for many emergency doctors. They compared high flow nasal cannula oxygen to facemask oxygen in palliative patients presenting to the emergency department with dyspnea. It was a cross-over trial, so all patients received both treatments. Dyspnea scores were 8 at baseline, 5 with the facemask oxygen, and 3 with HFNC. Objective measures, like respiratory rate, oxygen saturation, and use of morphine, also seemed to favour HFNC. I have been using this for years, but consistently run into bureaucratic problems. I am told that HFNC mandates an ICU admission, and that there is absolutely no flexibility despite the fact that these patients are palliative and their care will not be escalated no matter how they progress. That is obviously ridiculous, so I hope others work in places with administrators with more common sense.
Bottom line: There are obviously some limitations, which are discussed in the full blog post, but if you are not already using HFNC for palliation, I think this is good enough evidence to start.
The Evidence-Based Metaphor
Trogen B. The Evidence-Based Metaphor. JAMA. 2017 Apr 11;317(14):1411-1412. doi: 10.1001/jama.2016.17219. PMID: 28399255
“We implement evidence based medicine, so why not evidence based communication?”
We all spend an enormous amount of time memorizing facts, figures, biochemical pathways, and statistics. We are then tasked with explaining complex medical problems in simple, understandable language. To do so, we frequently make use of metaphors: cancer as an enemy or as a journey. The metaphors we use can have a tremendous impact on our patients’ interpretations of disease. Women who see breast cancer as the “enemy” are more likely to describe depression, anxiety, and a lower quality of life than those who saw their cancer as a “journey” or a “challenge”. This author argues that we need to understand the impacts of our language and ideally work to study and standardize the metaphors we use. I find this topic both fascinating and important. So many of the words we use when talking to our patients – severe, rare, heart failure, resuscitation – can easily be interpreted in novel and unexpected ways by our patients. There is no easy solution, but we must be cognizant of the possibility of miscommunication even when we are using relatively simple medical language.
The Mindset of the Resuscitationist
Gray SH, Lauria MJ, Hicks C. The Mindset of the Resuscitationist. Emerg Med Clin North Am. 2020 Nov;38(4):739-753. doi: 10.1016/j.emc.2020.06.002. Epub 2020 Jul 23. PMID: 32981614
I really can’t do justice to this paper in a summary – all 10 pages are pure gold. Considering the authors are Sara Gray, Michael Lauria, and Chris Hicks, that is not surprising at all. I am really just including the paper here as a reference, as I think many will find the content extremely high yield. I am not sure how wide this knowledge has spread in emergency medicine. For the FOAMed community, most of this article will seem fairly routine, but if you haven’t heard of a zero point survey, shared mental models, or failure friends, I would say this is an absolute must read.
Danish cowboys: Performing LPs with high INRs
Bodilsen J, Mariager T, Vestergaard HH, et al. Association of Lumbar Puncture With Spinal Hematoma in Patients With and Without Coagulopathy. JAMA. 2020 Oct 13;324(14):1419-1428. doi: 10.1001/jama.2020.14895. PMID: 33048155
This is a massive database trial looking at the association between coagulopathy (INR > 1.4, platelets < 150, or aPTT > 39 seconds) and the risk of spinal hematoma after lumbar puncture. Spinal hematoma occurred within 30 days in 0.2% of patients, whether or not there was coagulopathy. The only independent risk factors for hematoma were: male sex (HR 1.72), age 41-60 (HR 1.96), and age 61-80 (HR 2.20). Anticoagulation did increase the risk of a ‘traumatic tap’. As far as database studies go, this is as good as it gets. (It is based on a nationwide database in Denmark, and so had complete follow-up for more than 99% of patients). However, you can’t eliminate confounding. Why were the doctors willing to perform a lumbar puncture in someone with an elevated INR? Perhaps they only did it when they were sure it would be easy. Perhaps they only did it when the INR was elevated for liver disease, and therefore the patient wasn’t actually coagulopathic. It’s hard to know, but this data can’t really prove that coagulopathy is not a contraindication to LP. However, it does tell us that if you are very careful in your selection criteria, it is possible to safely perform LPs in coagulopathic patients. I just wish I knew what criteria these Danish doctors were using to select their patients.
Bottom line: In this database, there was no association between coagulopathy and spinal hematoma after lumbar puncture. I am certainly not using this data to LP indiscriminately, but if I think an LP is urgently needed, it is good to know that coagulopathy shouldn’t be an absolute contra-indication either.
Too big for CT?
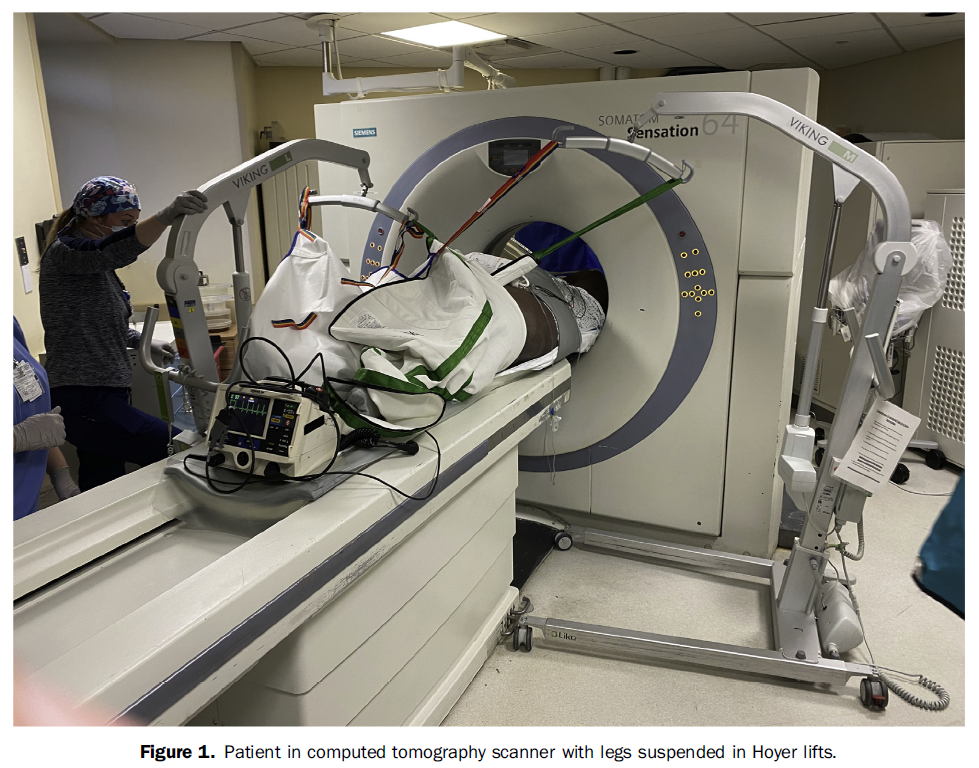
Sacchetti AD, Crookshank A, Leidy K. A Novel Solution to Patients Exceeding Weight Limit on Computed Tomography Scanner. Ann Emerg Med. 2021 Aug;78(2):313-314. doi: 10.1016/j.annemergmed.2021.04.012. PMID: 34325866
This case report from Al Sacchetti and colleagues is a little ridiculous, but also perhaps a little ingenious. They were caring for a patient with symptoms of a possible aortic dissection, but who weighed 485 pounds, and was therefore over the CT scanner’s 450 pound weight limit. They used 2 Hoyer lifts to suspend the patient’s legs, thus decreasing the total weight taken by the scanner, and they had good success. For some more objective measurements, they found a 400 pound volunteer, and by supporting the patient’s legs, the relative weight was only 325 pounds – a reduction of about 75 pounds or 18%. I think there is a lot that could go wrong here, so don’t like this as a regular solution. Really, we know that morbidly obese patients exist in our communities, and we know that these patients are likely to have medical problems that will require imaging.
Bottom line: Hospitals really need to consider the heaviest patients that could present, and not the average patient, when purchasing equipment (and manufacturers need to consider the same when building equipment).
Risk versus harm
Morgan DJ, Scherer LD, Korenstein D. Improving Physician Communication About Treatment Decisions: Reconsideration of “Risks vs Benefits”. JAMA. 2020 Sep 8;324(10):937-938. doi: 10.1001/jama.2020.0354. PMID: 32150219
This paper discusses a small but very important linguistic point. In medicine, we frequently talk about “risks versus benefits”, but that is an inherently biased comparison, implying that benefits are certain, but there is only a chance of harm. When discussing treatment options, it is important that our patients understand that there is only a possibility of benefit (and frequently it is a very small possibility, as illustrated by NNTs in the 100s for most treatments), and that possible benefit is balanced by possible harms. There are many studies that show that doctors have an inherent treatment bias – we believe our treatments are better and less harmful than they really are – and this language may play a subtle role in that bias. Being careful about our language can help ensure we don’t bias our patients’ decisions, and they get the best possible care. I like the example of a harm/benefit conversation they provide: “You have atrial fibrillation, and 4 of 100 people like you with atrial fibrillation will have a stroke every year. Let’s talk about the chance of benefits and harms of treatment with anticoagulation, which involves taking medication to decrease the ability of your blood to form clots. Studies have shown that treatment with these drugs reduces the chance of stroke occurring from 4 of 100 people with atrial fibrillation per year to 2 of 100 people per year. However, 1 to 3 people of 100 who are treated with these anticoagulation drugs will experience significant bleeding that could involve bleeding into the brain or intestinal tract. In other words, most patients like you do not benefit from or experience harms from this treatment.”
It’s all about perception
Abidova A, Alcântara da Silva P, Moreira S. Accuracy of Patients’ Waiting Time Perceptions in the Emergency Department. Acad Emerg Med. 2020 Dec;27(12):1348-1349. doi: 10.1111/acem.13949. Epub 2020 Mar 18. PMID: 32103560
As healthcare systems around the world strain after a second year of pandemic, this paper about wait times in the emergency department might be particularly timely. This is a retrospective study, with essentially no methods section, so I don’t trust the numbers at all, but I think the general message is correct: the majority of patients overestimate the amount of time that they have been waiting. (76% of patients over-estimated their wait times, 20% were accurate, and a small number under-estimated). I don’t think that is novel information, but it is something we should think about, and I think we generally come at this from the wrong perspective in emergency medicine. For the most part, we just blame the patients and call them dumb. Patients will complain that they have been waiting for 2 hours, and will be met with the response, “no, dummy, the computer says you have only been waiting 1.5 hours.” The key point is that the patient feels like they have been waiting 2 hours, and that is largely our fault. There are lots of ways that we could influence the perception of wait times, but we routinely fail. Personally, I hate waiting, but how much I hate waiting is extremely relative. The last time I was in the emergency room as a patient, I sat in an extremely uncomfortable chair, with no available food or drink, jammed right between a elderly man continuously vomiting and a drunk woman screaming at everyone. I had no idea how long I would have to wait, there was no cel service or wifi, and the battery on my phone was rapidly falling with nowhere available to charge it. I was miserable. Conversely, the last time I had to wait for my car to be repaired, I was seated in a comfortable chair, provided with a wifi password and a coffee, and received frequent updates about the expected time remaining. Objectively, these researchers would have told me the time I spent waiting in both settings was identical, but if that is their conclusion, I can tell you objectively that they are wrong. (And this is ignoring the added anxiety of waiting in an ED for a possible life-threatening illness). It has never been a huge priority, but I think we need to rethink HOW patients wait, not just how long they wait.
Hypothermia not looking so hot anymore
Dankiewicz J, Cronberg T, Lilja G, et al: TTM2 Trial Investigators. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. N Engl J Med. 2021 Jun 17;384(24):2283-2294. doi: 10.1056/NEJMoa2100591. PMID: 34133859
In many ways, ‘therapeutic’ hypothermia is not unlike thrombolytics for ischemic stroke: there were two small positive trials, but they had numerous sources of bias, so the scientific community remained skeptical while the rest of the medical world rapidly implemented a relatively unproven therapy (at tremendous cost). The TTM 2 trial randomized 1861 comatose patients with ROSC after out of hospital cardiac arrest to either hypothermia (33 degrees Celsius) or normothermia (a target of less than 37.5 degrees Celsius). There was no difference in mortality (their primary outcome), nor in neurologic outcomes. The only difference was an increase in arrhythmias resulting in hemodynamic compromise in the hypothermia group (24% vs 16%, p<0.001).
Bottom line: After the pair of TTM trials, we know for sure that hypothermia is not beneficial. Whether fever control, or any temperature management, is effective remains an open question, but that is a hypothesis untested by RCTs. Based on data in other critically ill patients, it is very unlikely that fever control improves outcomes, but I imagine we will see RCTs on that in the future.
The full write up can be found here.
Cheesy Jokes of the Month
Who hides in the bathroom at parties?
The party-pooper
Morgenstern, J. Research Roundup (August 2021), First10EM, August 16, 2021. Available at:
https://doi.org/10.51684/FIRS.83756

2 thoughts on “Research Roundup (August 2021)”