Doctors prescribe a lot of antibiotics for viral illness. We shouldn’t do that. Antibiotics don’t work for viral illnesses, but for some reason many doctors can’t seem to help themselves. Because of all this inappropriate prescribing, someone came up with the (not so) brilliant idea of delayed antibiotic prescriptions, in that you still prescribe the completely unnecessary medication, but just ask the patient nicely not to take it for a few days. When compared to handing out antibiotics like candy, delayed prescriptions might sound like a good idea, but when compared to just being good doctors and only prescribing antibiotics as appropriate, delayed prescriptions are patently ridiculous. There is already plenty of data that demonstrates exactly how delayed prescriptions work, but I decided to include a brief summary of a new RCT because I have seen it cited in many locations as a win for delayed antibiotics, when in fact it clearly demonstrates harm from the practice.
The paper
Mas-Dalmau G, Villanueva López C, et al. Delayed Antibiotic Prescription for Children With Respiratory Infections: A Randomized Trial. Pediatrics. 2021 Mar;147(3):e20201323. doi: 10.1542/peds.2020-1323. Epub 2021 Feb 11. PMID: 33574163
The Methods
This is a a multicenter randomized clinical trial to compare 3 antibiotic treatment strategies for children with acute uncomplicated RTIs.
Patients
Patients aged 2-14 years attending a primary care pediatrician’s office with their parent for one of: pharyngitis, rhinosinusitis, acute bronchitis, or acute otitis media.
- Pediatricians had to have reasonable doubt about the need for antibiotics
Intervention and comparison
The trial had three arms:
- Delayed antibiotic prescription
- A prescription was given immediately, but parents were advised not to give it unless:
- The child did not start to feel better after 4, 7, 15, or 20 days from symptom onset for acute otitis media, pharyngitis, rhinosinusitis, or acute bronchitis, respectively
- The child had a temperature of >39°C after 24 hours or a temperature of >38°C but <39°C after 48 hours
- The child felt much worse
- A prescription was given immediately, but parents were advised not to give it unless:
- Immediate antibiotic prescription
- No antibiotic prescription
Outcome
The primary outcomes (you really shouldn’t have more than one) were severity and duration of respiratory infection symptoms over 30 days.
The Results
They included 436 patients. The mean age was 6 and half were females. The majority of infections were either pharyngitis or otitis media. About half of patients rated their symptoms as severe on the first visit.
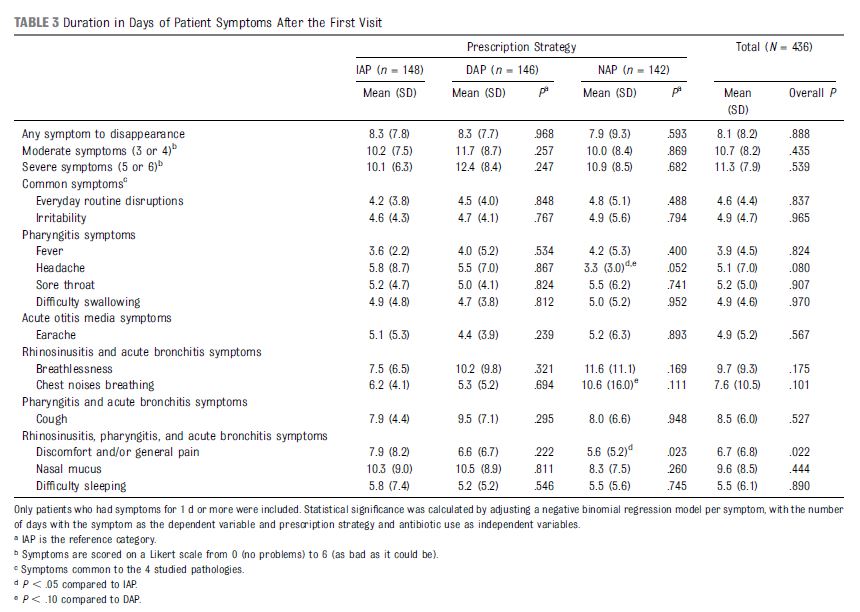
There were no differences in their primary outcomes. The mean duration of any symptoms was 8.3 days with delayed antibiotics, 8.3 days with immediate antibiotics, and 7.9 days with no antibiotics.
Across the board, there are no differences in the large number of symptoms that they measured. There was only one statistically significant finding, and that group favoured faster resolution of pain in the no antibiotic group, but is almost certainly a chance finding from multiple comparisons. There were more gastrointestinal side effects in the immediate antibiotics group (8.8% versus 3.4% delayed and 2.8% no antibiotics).
Antibiotic use was heavily determined by the action of the doctor. 96% of the immediate antibiotic group took antibiotics, as compared to 25% of the delayed antibiotic group, and 12% of the no antibiotic group (all statistically significant).
There were no differences in complications, unscheduled visits, or satisfaction.
My thoughts
The results of this trial are the same as for every delayed antibiotic trial. There are no differences in complications. Delayed antibiotics decrease antibiotic use as compared to an immediate antibiotic strategy, but increase antibiotic use as compared to appropriate care (no antibiotics when they aren’t indicated). The more antibiotics that are used, the more side effects that are seen.
For some reason, people love to focus on the comparison between delayed antibiotics and inappropriate care (immediate antibiotics). In that comparison, delayed antibiotics look great. But if you compare anything to a control group that you know is getting inappropriate care, it will end up looking great. It isn’t an appropriate comparison.
When compared to appropriate care (not prescribing antibiotics when they aren’t indicated), delayed antibiotics are harmful, increasing overall antibiotic use with no benefit.
The outcomes are probably even worse than they seem at first glance. This is obviously not a blinded trial, and the primary outcome is subjective, which significantly increases the chance of bias. That bias will almost certainly make antibiotics look better than they really are. This is reflected in the fact that parents who received antibiotics were much more likely to believe the antibiotics were effective in making their child better (even though they weren’t). In other words, they actually measured very significant bias in their secondary outcomes. Despite that bias, the actual symptoms were rated identically in all three groups. Therefore, if you consider the expected bias among patient receiving antibiotics in this unblinded trial, it is possible (or perhaps even likely) that symptoms were actually worse among patients receiving antibiotics (whether immediate or delayed).
Antibiotics cause side effects. There are the immediate consequences: 1 in 11 kids in this trial developed GI side effects. There are also long terms consequences, such as antibiotic resistance. That will never who up in a short term RCT, but as we progress towards a potential post-antibiotic world, where rampant resistance limits our ability to treat basic infections, it is an outcome we should all consider.
The results of this trial are very clear, as long as you pick the appropriate comparison group. As compared to quality medical care, in which antibiotics are not prescribed when they are not needed, delayed antibiotic prescriptions increase antibiotic use (and therefore harm) without any clinical benefit.
Bottom line
This RCT shows that both delayed antibiotic and immediate antibiotic prescription strategies are worse than appropriate medical care, in which antibiotics are only prescribed when medically indicated. (Antibiotics don’t magically start treating viruses just because you wait 2 days.)
Other FOAMed
Delayed antibiotics are (mostly) dumb
References
Mas-Dalmau G, Villanueva López C, et al. Delayed Antibiotic Prescription for Children With Respiratory Infections: A Randomized Trial. Pediatrics. 2021 Mar;147(3):e20201323. doi: 10.1542/peds.2020-1323. Epub 2021 Feb 11. PMID: 33574163
Photo by Mauro Tchorbadjian on Unsplash
Morgenstern, J. Another study demonstrating the harms of delayed antibiotics, First10EM, July 19, 2021. Available at:
https://doi.org/10.51684/FIRS.79188


2 thoughts on “Another study demonstrating the harms of delayed antibiotics”
You have to examine the results of no antibiotic prescription in otitis media streptococcal pharyngitis with fusiform and bronchitis due to mycoplasma and bordetella pertussis