
Morgenstern, J. No, metformin is probably not the cure for long COVID, First10EM, June 19, 2023. Available at:
https://doi.org/10.51684/FIRS.130676
The internet is alive with rumors of a simple, cheap, low-risk cure for long COVID. Sound too good to be true? That’s because it almost certainly is. Let’s talk about this COVIT-OUT trial and what it says about metformin.
The paper
Bramante CT, Buse JB, Liebovitz DM, et al. Outpatient treatment of COVID-19 and incidence of post-COVID-19 condition over 10 months (COVID-OUT): a multicentre, randomised, quadruple-blind, parallel-group, phase 3 trial. Lancet Infect Dis. 2023 Jun 8:S1473-3099(23)00299-2. doi: 10.1016/S1473-3099(23)00299-2. PMID: 37302406 NCT04510194
The Methods
This is a publication looking at a “key secondary outcome” of a trial that was already published, and which had negative results. (Bramante 2022) Despite being described as a “key secondary outcome”, they state that long COVID was not a known entity when the trial started, and this outcome was therefore added partway through data collection. This publication looks at 300 day outcomes, based on survey responses. This was a decentralized trial, with no in-person contact with patients. Study drugs were mailed to participants.
Patients
Patients were recruited through online advertising. They included adult patients between the ages of 30 and 85 who were overweight or obese, and had confirmed COVID with symptoms for fewer than 7 days.
Patients were excluded if they were already on any of the study drugs, on any FDA approved treatment for COVID, or they never received a dose of the study drug. Vaccination status was not part of the inclusion criteria, and interestingly, they included pregnant women.
Intervention / Comparison
There are 6 groups in this trial:
- Metformin plus ivermectin
- Placebo plus ivermectin
- Metformin plus fluvoxamine
- Placebo plus fluvoxamine
- Metformin plus placebo
- Placebo plus placebo
The metformin was dosed as: 500mg on day one, 500 mg BID on day 2-5, and then 500mg in the morning and 1000 mg in the evening up to day 14.
The ivermectin was dosed as 390–470 μg/kg per day for 3 days (median 430 μg/kg per day). They don’t indicate in this manuscript how they were able to do weight based dosing with the opaque pre-prepared medication packages described.
The fluvoxamine was dosed as 50 mg on day one and then 50 mg BID until day 14.
Outcome
The trial’s primary outcome was severe COVID-19 by day 14 (and there was no benefit from any medication). (Bramante 2022) I will also note that although they say this was their original primary outcome, their initial clinicaltrials.gov submission had 4 completely different primary outcomes, which is a massive red flag.
This publication looks at the secondary outcome of self-reported long COVID diagnosis made by a medical provider.
The Results
They screened 6602 patients and included 1323 in the original trial, and 1126 are left in the long term survey data. If you are thinking about applying these results, beware of the long list of exclusions, all of which are hidden in supplemental material. This is in addition to the selection bias that occurs because people who respond to internet ads to participate in medical research are not like the general population. (But that probably doesn’t matter, because I don’t think you should apply these results clinically.)
The median age was 45, median BMI was 30, 56% were female, and 7% were pregnant. 8.3% of the total population reports being given a long COVID diagnosis.
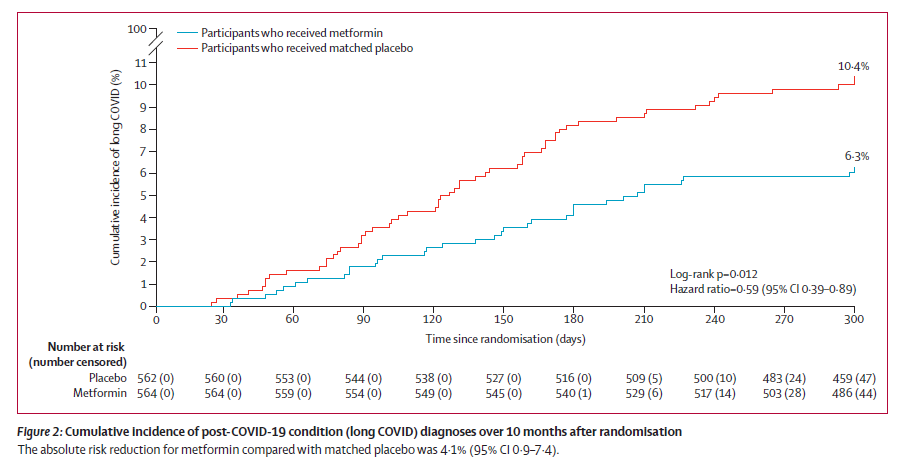
Long COVID was reported in 6·3% (95% CI 4·2–8·2) of participants who received metformin and 10·4% (7·8–12·9) of those who received matched placebo (HR 0·59, 95% CI 0·39–0·89; p=0·012).
There was no reported benefit for either ivermectin or fluvoxamine. Long COVID was reported in 7·7% (95% CI 5·0–10·4) of participants who received ivermectin and 8·1% (5·3–10·9) of those who received matched placebo (HR 0·95, 95% CI 0·57–1·59). Rates were 10·1% (95% CI 6·6–13·5) in participants who received fluvoxamine and 7·5% (4·4–10·4) in those who received matched placebo (HR 1·36, 95% CI 0·78–2·35).
Long COVID rates were 10.3% among unvaccinated patients (507 total), 6.6% among patients with the primary series (619), and 1.8% in patients with a booster (57).
My thoughts
This is clearly not a practice changing publication, for many reasons.
When given an independent publication, it is tempting to treat this like an independent trial, but this publication is really just a look at a secondary outcome of a negative trial, and I think it should be treated exactly like we treat all secondary outcomes (especially when they are discordant with the primary outcome of the trial). (Bramante 2022) This is especially true with this trial, because the secondary outcome of interest wasn’t added until well after the trial was started. This is hypothesis generating, but not practice changing.
As I said in some of my very first COVID posts, when the scientific community is throwing absolutely everything at the COVID wall, a few things are bound to stick by chance alone. There is little reason to think a priori that metformin would be effective against a viral respiratory illness. (They will justify its choice by changes in inflammatory markers, but essentially every drug has some effect on inflammatory markers, in one way or another. Emphasizing these markers to match your hypothesis is a classic pseudoscience trope.) We need to adjust our pretest probability down based on the sheer number of agents tested against COVID without the normal theoretical basis.
Although we clearly don’t understand long COVID, I think we also need to lower our pretest probability when the agent had no effect on the primary outcome during the acute phase of the infection. (Bramante 2022) Negative results were also seen in the TOGETHER trial, which demonstrated no difference between metformin and placebo. (Reis 2022) How do you explain benefits months later without any benefit originally? (Although, apparently this happens with thrombolytics and stroke. Take that as you will.) In this case, there were some secondary outcomes in the original trial that were statistically positive, but they also need to be assessed as the secondary outcome they are. I will also admit that the acute studies are looking for markers of severe COVID, whereas long COVID does not seem to be associated with severity of disease, so the lack of early effect is not as damning as it would be with something like ischemic stroke.
I have heard people argue that this study proves that long COVID has physiologic (rather than psychological) origins, but that argument overlooks the most likely explanation: a chance finding.
The outcome of this study is entirely based on survey data. It is also looking at a diagnosis that has no clinical gold-standard. I would expect this outcome to be incredibly unreliable. That being said, this trial was completely blinded, which should help limit the many sources of bias that occur when such an unreliable outcome is used.
This study has a number of other unusual features that make it harder to appraise. For example, for the first 6 months, it was a pure trial of metformin versus placebo. They added all the other groups later. Adaptive trials were the rage during COVID, and there are good reasons for them, but the more changes that are made, the more cracks open up for bias to seep in.
I wonder whether the placebo numbers give us a sense that this is a spurious finding. The rate of long COVID was 10.4% in the metformin placebo group, 8.1% in the ivermectin placebo group, and 7.5% in the fluvoxamine placebo group. In other words, the big difference here seems to be among the placebo groups, and therefore perhaps not the result of active treatment? (However, this is somewhat complicated, as the placebo groups contain people taking the other active ingredients, which would make them less like placebo if any of these therapies actually worked.)
I love it when I see biases creep into research in new and unusual ways. This trial is a really interesting example of publication or reporting bias. I heard about this trial through multiple channels, but it wasn’t until I downloaded the manuscript myself that I became aware that ivermectin and fluvoxamine were also studied. We have an incredible ability to magnify potentially positive results, while simultaneously ignoring negative results. Even the publication itself is biased in this way. The charts and graphs literally only mention metformin, with the two other agents just briefly mentioned in the text. (This is especially striking when contrasted to the initial publication from this study, which was clearly negative for all agents, and featured all three agents equally). (Bramante 2022)
I think it is very clear that this treatment is not ready for clinical use. I have seen many contrary opinions. Twitter was full of voices emphasizing how safe and cheap metformin is, and therefore suggesting widespread adoption. Even putting aside the many reasons not to trust these results, I think that logic fails dramatically. Although metformin itself might be cheap, identifying patients with COVID is not. We now (thankfully) live in a world where only a small minority of viral infections are COVID. In order to implement therapies for COVID, we will have to screen dozens, and perhaps hundreds, of patients to find one eligible. However, we don’t live in a world where the healthcare infrastructure is set up to test every patient with a viral syndrome. This is a massive factor that proponents of metformin therapy seem to be overlooking. If you want to treat widely with metformin, you are going to be pushing scores of patients (who don’t otherwise need emergency care) to the emergency department, just for testing and treatment with a yet unproven therapy. Let’s at least get some solid proof of benefit before adding this astronomical cost to our already over-stretched healthcare systems.
Bottom line
This paper presents the secondary outcome of a previously published trial, and generates the hypothesis that metformin could decrease rates of long COVID. It clearly should not be used to change clinical practice.
Other FOAMed
Inside Medicine: Did a clinical trial just “prove” that Long Covid really exists?
References
Bramante CT, Huling JD, Tignanelli CJ, Buse JB, Liebovitz DM, Nicklas JM, Cohen K, Puskarich MA, Belani HK, Proper JL, Siegel LK, Klatt NR, Odde DJ, Luke DG, Anderson B, Karger AB, Ingraham NE, Hartman KM, Rao V, Hagen AA, Patel B, Fenno SL, Avula N, Reddy NV, Erickson SM, Lindberg S, Fricton R, Lee S, Zaman A, Saveraid HG, Tordsen WJ, Pullen MF, Biros M, Sherwood NE, Thompson JL, Boulware DR, Murray TA; COVID-OUT Trial Team. Randomized Trial of Metformin, Ivermectin, and Fluvoxamine for Covid-19. N Engl J Med. 2022 Aug 18;387(7):599-610. doi: 10.1056/NEJMoa2201662. PMID: 36070710
Bramante CT, Buse JB, Liebovitz DM, Nicklas JM, Puskarich MA, Cohen K, Belani HK, Anderson BJ, Huling JD, Tignanelli CJ, Thompson JL, Pullen M, Wirtz EL, Siegel LK, Proper JL, Odde DJ, Klatt NR, Sherwood NE, Lindberg SM, Karger AB, Beckman KB, Erickson SM, Fenno SL, Hartman KM, Rose MR, Mehta T, Patel B, Griffiths G, Bhat NS, Murray TA, Boulware DR. Outpatient treatment of COVID-19 and incidence of post-COVID-19 condition over 10 months (COVID-OUT): a multicentre, randomised, quadruple-blind, parallel-group, phase 3 trial. Lancet Infect Dis. 2023 Jun 8:S1473-3099(23)00299-2. doi: 10.1016/S1473-3099(23)00299-2. Epub ahead of print. PMID: 37302406
Reis G, Dos Santos Moreira Silva EA, Medeiros Silva DC, Thabane L, Cruz Milagres A, Ferreira TS, Quirino Dos Santos CV, de Figueiredo Neto AD, Diniz Callegari E, Monteiro Savassi LC, Campos Simplicio MI, Barra Ribeiro L, Oliveira R, Harari O, Bailey H, Forrest JI, Glushchenko A, Sprague S, McKay P, Rayner CR, Ruton H, Guyatt GH, Mills EJ. Effect of early treatment with metformin on risk of emergency care and hospitalization among patients with COVID-19: The TOGETHER randomized platform clinical trial. Lancet Reg Health Am. 2022 Feb;6:100142. doi: 10.1016/j.lana.2021.100142. Epub 2021 Dec 14. PMID: 34927127
Photo by Christina Victoria Craft on Unsplash



3 thoughts on “No, metformin is probably not the cure for long COVID”
Thank you
JM – do you think its poss the benefit, if real, was due to untreated metabolic syndrome patients who got a little weight-loss/metabolic boost that metformin reportedly gives people…and so they were less likely to experience the “i still dont feel good” syndrome of long covid?
There are certainly lots of reasons that metformin might be beneficial in a population of overweight and obese patients, especially in a country with imperfect access to primary care. That being said, I think the most like explanation (Like it is for almost all secondary outcomes that are outliers from the rest of the study) is that this is just a mathematical chance finding that will never be reproduced. We get a lot of these in medicine, because we use a ridiculously low statistical bar as compared to other areas of science.