Ren, D. Christmas in July: New Guidelines for Managing Well-appearing Febrile Infants from the American Academy of Pediatrics, First10EM, September 6, 2021. Available at:
https://doi.org/10.51684/FIRS.86494
I will live in the Past, the Present, and the Future. The Spirits of all Three shall strive within me. I will not shut out the lessons that they teach.
A Christmas Carol by Charles Dickens
Feels like Christmas came early this year, with the American Academy of Pediatrics gifting us a set of clinical practice guidelines for evaluating and managing the well-appearing febrile infant:
Pantell RH, Roberts KB, Adams WG, et al. Evaluation and management of well-appearing febrile infants 8 to 60 days old. Pediatrics. 2021;148(2):e2021052228. PMID: 34281996 [full text]
In addition to 3 new algorithms and 21 key action statements, these new guidelines include a brief historical account of our journey in managing the febrile infant and some positing of what is yet to come.

This is a guest post by Dr. Dennis Ren. Dennis is currently a pediatric emergency medicine fellow at Children’s National Hospital in Washington, DC. He has been a guest on podcasts such as Peds Admit and The Skeptics’ Guide to Emergency Medicine. His areas of interest include medical education, simulation, interprofessional communication and teamwork, disaster/emergency preparedness.
Inclusion and Exclusion Criteria
| Included | Excluded |
|---|---|
| Well appearing Rectal temperature ≥38°C (100.4°F) at home in past 24 hours or in clinical setting | Preterm <37 weeks gestation |
| Gestational age ≥37 and <42 weeks | <2 weeks with perinatal course complicated by maternal fever, infection, and/or antimicrobial use |
| Age 8 to 60 days | High suspicion of HSV |
| Home after discharge from newborn nursery or born at home | Focal bacterial infection |
| Can also include: respiratory symptoms, diarrhea, otitis media, current/recent use of antimicrobials if >2 weeks, positive respiratory viral test | Clinical bronchiolitis |
| Immune compromise | |
| Neonatal course complicated by surgery\infection | |
| Medically fragile or technology dependent | |
| Immunizations within 48 hours |
Ghost of Guidelines Past
We have been at this for more than 40 years. Previously, some institutions would perform a full sepsis workup (blood, urine, cerebrospinal fluid) for anyone under 90 days of age. Criteria based on subjective findings and predetermined laboratory testing thresholds were created to help identify low risk infants. However, with improvements in food safety, screening during pregnancy, and introduction of conjugate pneumococcal vaccination, the rates of Listeria, Group B streptococcus, and Streptococcus pneumoniae have declined. Thus, there has been a shift from Gram-positive to Gram-negative organisms being primarily responsible for bacterial infections in this age group. The scary part is that application of previous criteria in the current era may miss close to one-third of infants with bacterial meningitis.
In general, the risk of bacteremia and bacterial meningitis declines with age, but how low can we go in terms of age at which we still need to perform the full versus partial work up?
Ghost of Guidelines Present
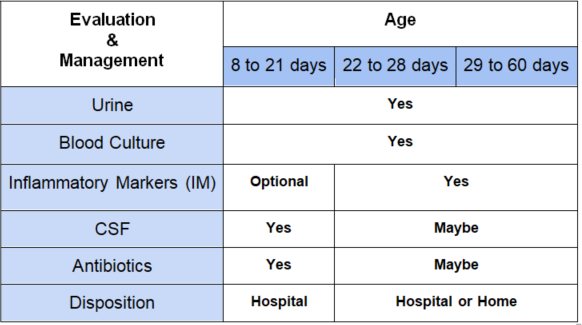
4 Key Components of Evaluation
| Urine | Blood Culture | Inflammatory Markers (IM): Procalcitonin>0.5 ng/mL; Absolute neutrophil count (ANC)>4000 mm3, >5200 mm3;CRP >20 mg/L; Temperature > 38.5°C | Cerebrospinal Fluid (CSF) |
(There are two ANC cutoffs included based on the PECARN study and Febrile Young Infant Research Collaborative study.)
The authors recommend using procalcitonin and either ANC or CRP. If procalcitonin is not available or results will not be reported in a timely manner, use a combination of ANC, CRP, and temperature.
Algorithms at a Glance
0 to 7 days
The authors made the decision to not include this age group in the guidelines, citing that there were different rates and types of illness. For this age group, I would be hard pressed not to perform a complete workup (blood, urine, CSF) on any infant with a fever.
8 to 21 days
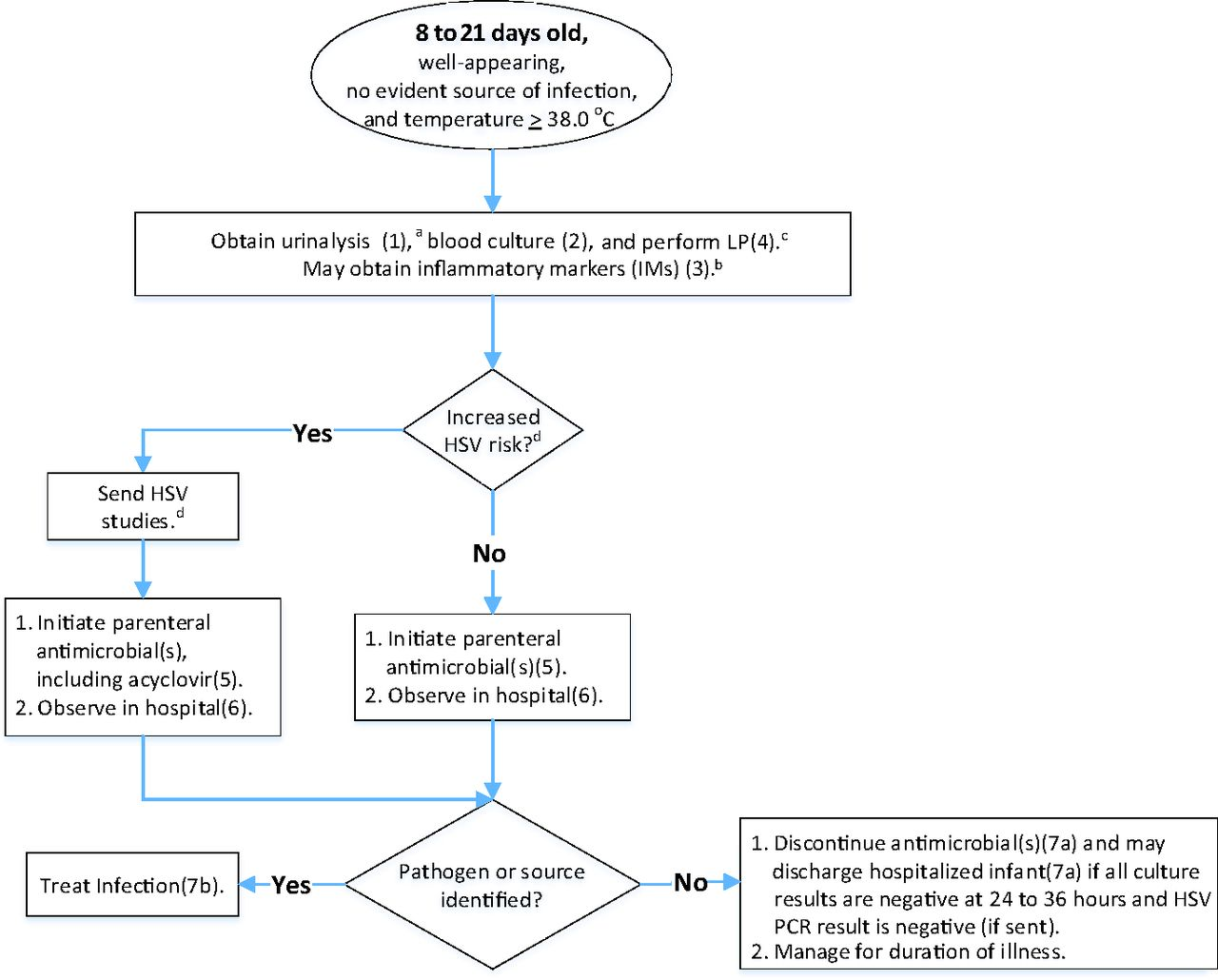
There is not much deviation from typical practice in this age group. We should continue to be conservative, with all febrile infants receiving a complete work up. Adding the inflammatory markers is a soft recommendation as it really does not change your work up or disposition in the emergency department. All infants in this age group should be treated with antibiotics and observed in the hospital. There is a special word of caution here about identifying risk factors for herpes simplex virus (HSV) as that would require the addition of acyclovir.

Consider HSV if:
- Maternal history of genital HSV lesions or fevers 48 hours before or after delivery
- Vesicles
- Seizures
- Hypothermia
- Mucous membrane ulcers
- CSF pleocytosis without positive Gram stain
- Leukopenia
- Thrombocytopenia
- Elevated alanine aminotransferase levels
Recommended HSV studies:
- CSF PCR
- HSV surface swabs from mouth, nasopharynx, conjunctivae, and anus for HSV culture or PCR assay
- Alanine aminotransferase
- Blood PCR
The algorithms for these next two age groups allow for some more flexibility and shared decision making.
22 to 28 days
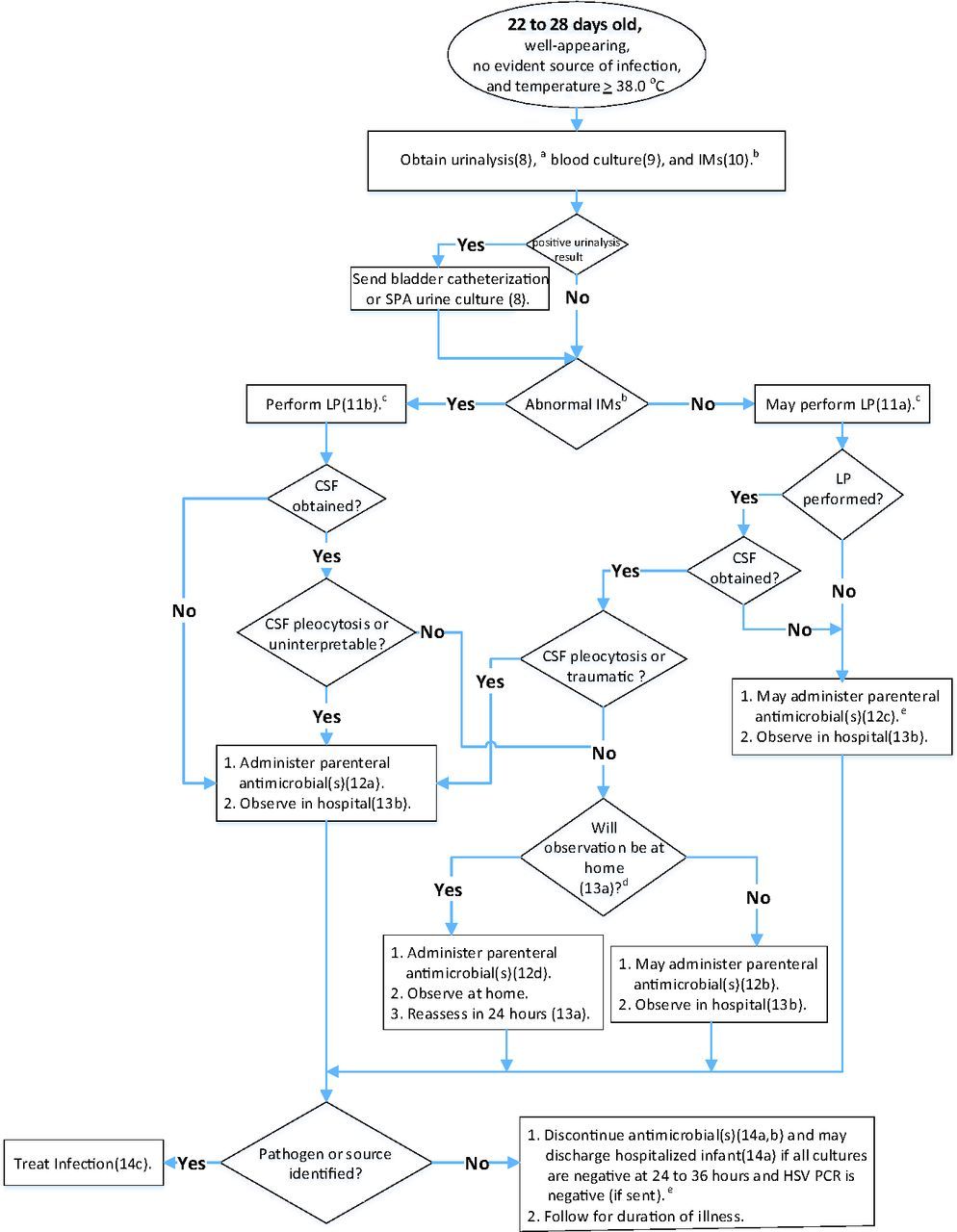
This age group should have urine, blood culture, and IMs obtained. The IMs will guide decision-making about whether or not to pursue LP and obtain CSF. If the IMs are abnormal, LP should be obtained. If the IMs are normal, LP may still be obtained. If CSF is obtained and there are no signs of infection, the infant should be given a dose of empiric antibiotics and may be sent home with close follow up within 24 hours. A key point in this age group is that if CSF is not obtained or uninterpretable, these patients should NOT be sent home. If the decision is made to defer LP, the patient should be hospitalized and observed. Just know if antibiotics are administered without CSF results, there is a risk of partially treated meningitis.
29 to 60 days
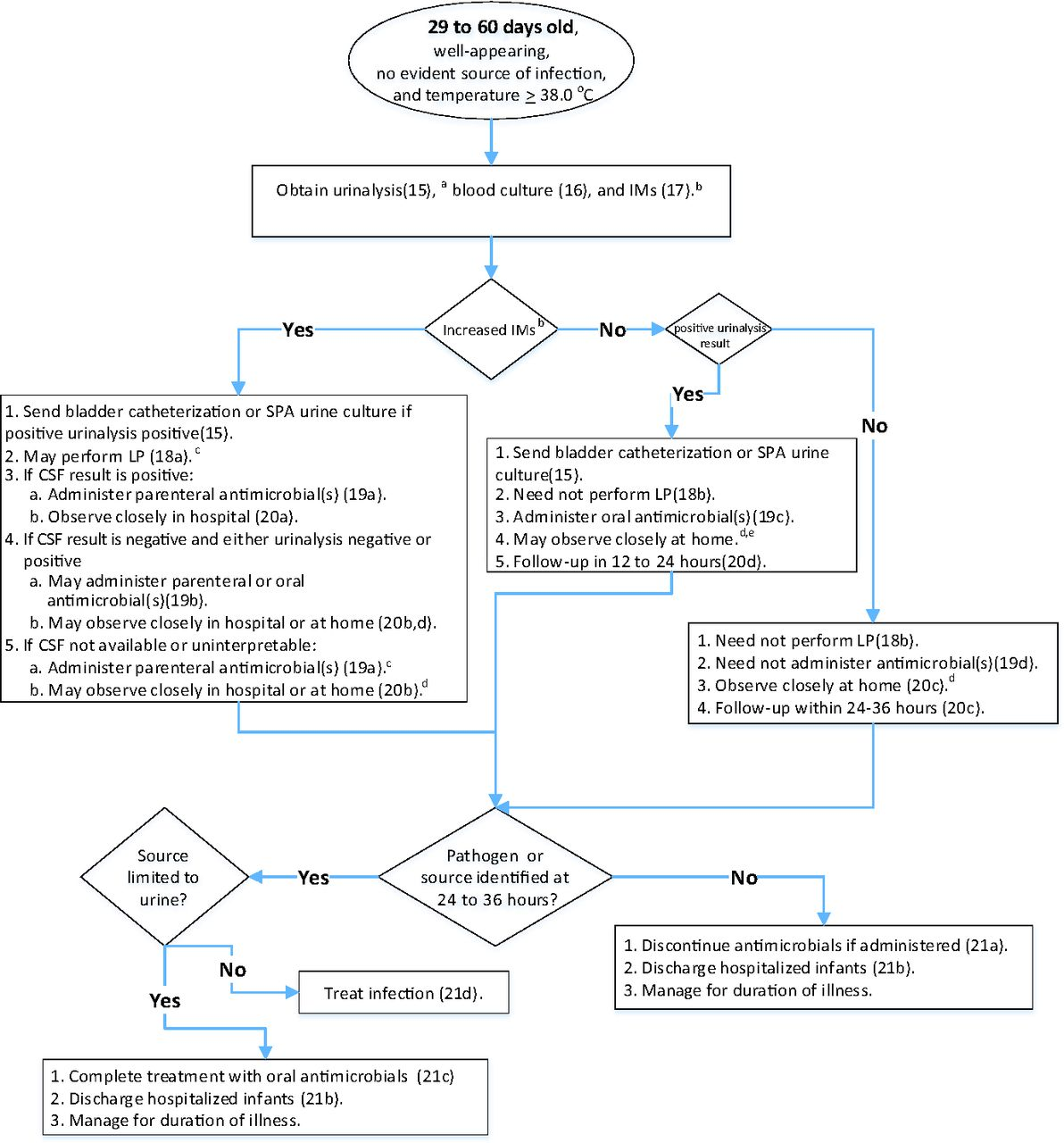
This age group has the most room for shared decision making between the clinician and the family and has potential to decrease LPs and let us send more infants home. It still recommends starting with urine, blood, and IMs. In this age group, if all IMs are normal, the patient can be discharged home. With normal IMs and a positive urinalysis, they go home on oral antibiotics with follow up in 12 to 24 hours. With normal IMs and a negative urinalysis, they can even be sent home without antibiotics with follow up in 24 to 36 hours.
In the case that IMs are abnormal, things get a bit more complex. The guidelines say that an LP may be performed. Note that this is different from the previous age group which said that an LP should be performed in anyone with abnormal IMs. Obviously, if the CSF results are positive, these infants are receiving antibiotics and being hospitalized. However, if the CSF results are negative with either a positive or a negative urinalysis, there is room for discussion regarding oral vs. parenteral antibiotic treatment and disposition home vs. hospital. If the CSF is not obtained or uninterpretable, the guidelines suggest administering parenteral antibiotics but the infant may be hospitalized or discharged home with close observation.
Make sure to have a thorough discussion with the family regarding the risks and benefits of the decision, provide strict return precautions, and emphasize the importance of follow up.
Ghost of Guidelines Future
With these new guidelines, we have made a bit more progress towards lowering the age at which well-appearing febrile infants receive a full workup including blood, urine, and CSF. There are a few things to note moving forward:
Age is but a Number
Overall, rates of bacteremia and bacterial meningitis decline with age. However, these age cut offs are arbitrary. Is there truly a big difference between infants 28 vs 29 days old? The best decision for evaluation and management may vary on a case by case basis, taking into account the risk tolerance or aversion of the clinician and family along with clinical judgement and the available scientific evidence.
No More “SBI”
Traditionally, everything (urinary tract infection, bacteremia, bacterial meningitis, etc) was lumped into one category, “SBI.” Going forward, we should stop using this term and be specific about the type of infection. Urinary tract infections are much more common than bacteremia and bacterial meningitis so may confound accuracy of prediction models. Similarly, bacterial meningitis is so rare that finding a large enough sample is difficult. If we strive to be specific with what we are evaluating, maybe we will develop clinical prediction rules that can be applied to different types of infections.
Stop using WBC
These guidelines offer multiple options for IMs. Their preference is using procalcitonin with either CRP or ANC. If procalcitonin is not available or the results are not accessible in a reasonable time, they recommend a combination of ANC, CRP, and temperature >38.5°C. No isolated IM is reliable for risk stratification. They recommend against using WBC for risk stratification.
Remember that although these guidelines incorporate evidence from some validated tools like PECARN or Step-by-Step, they still need to be prospectively validated. Until then, “God bless us, every one!” (I’m sorry. I just could not resist.)
References
- Lyons TW, Garro AC, Cruz AT, et al. Performance of the modified boston and philadelphia criteria for invasive bacterial infections. Pediatrics. 2020;145(4):e20193538.
- Kuppermann N, Dayan PS, Levine DA, et al. A clinical prediction rule to identify febrile infants 60 days and younger at low risk for serious bacterial infections. JAMA Pediatr. 2019;173(4):342-351.
- Aronson PL, Shabanova V, Shapiro ED, et al. A prediction model to identify febrile infants ≤60 days at low risk of invasive bacterial infection. Pediatrics. 2019;144(1):e20183604.
- Gomez B, Mintegi S, Bressan S, et al. Validation of the “step-by-step” approach in the management of young febrile infants. Pediatrics. 2016;138(2):e20154381.
Other FOAMed
To LP, or not to LP (the febrile infant): That is the question
If you want to read a little more about what makes a good or bad guidelines (this guidelines has a mix of both), see this post: I hate guidelines
Skeptics’ Guide to Emergency Medicine
Don’t Forget the Bubbles
emDocs: Small Talk- Hot Off the Presses: The Latest AAP Guidelines for the Febrile Neonate
Pediatric EM Morsels: Febrile Infants 8 to 28 Days Old! Pediatric Fever Update
Pediatric EM Morsels: Febrile Infants 29 to 60 Days Old!
Ren, D. Christmas in July: New Guidelines for Managing Well-appearing Febrile Infants from the American Academy of Pediatrics, First10EM, September 6, 2021. Available at:
https://doi.org/10.51684/FIRS.86494
Photo by 🇸🇮 Janko Ferlič on Unsplash