
Although emergency medicine is an incredibly rewarding profession, it is undeniably marked by significant levels of stress. (Stress levels are at an all time high during COVID-19, but this is not a COVID post, so that is the last I will mention it.) Burnout levels are higher in emergency medicine than most other areas of medicine, and burnout is associated with a loss of empathy and compassion towards patients, decreased job satisfaction, and shorter careers in medicine. (Bragard 2015, Li 2018, Lu 2015, Bellolio 2014) There is some prior research that suggests that exposure to animals can decrease stress. (Barker 1998; Lundqvist 2017) This quick post looks at a paper by Kline and colleagues exploring the potential for dog therapy (and art therapy as well, but that interests me much less) to reduce stress during an emergency department shift.
The paper
Kline JA, VanRyzin K, Davis JC, et al. Randomized Trial of Therapy Dogs Versus Deliberative Coloring (Art Therapy) to Reduce Stress in Emergency Medicine Providers . Acad Emerg Med. 2020; doi:10.1111/acem.13939 PMID: 32266765 [article] NCT03628820
The Methods
This is a prospective, single-center, controlled trial looking at effects dog therapy and art therapy during an emergency department shift.
Patients
Emergency care providers, including nurses, residents, and physicians, from a single center emergency department.
- Exclusions: Dislike, allergy, fear, or other reason not to interact with a therapy dog.
Interventions
Dog therapy: consisted of an interaction with a therapy dog, which providers could pet or touch as they wished.
Art therapy: consisted of colouring one of three mandalas (patterns) with a provided set of coloring pencils.
Both of these activities occurred about halfway through the provider’s shift, in a quiet room, physically separated from the clinical care area, with no electronic devices, telephone, window, or overhead speaker.
Comparison
A convenience sample of providers that were not offered any break.
Outcome
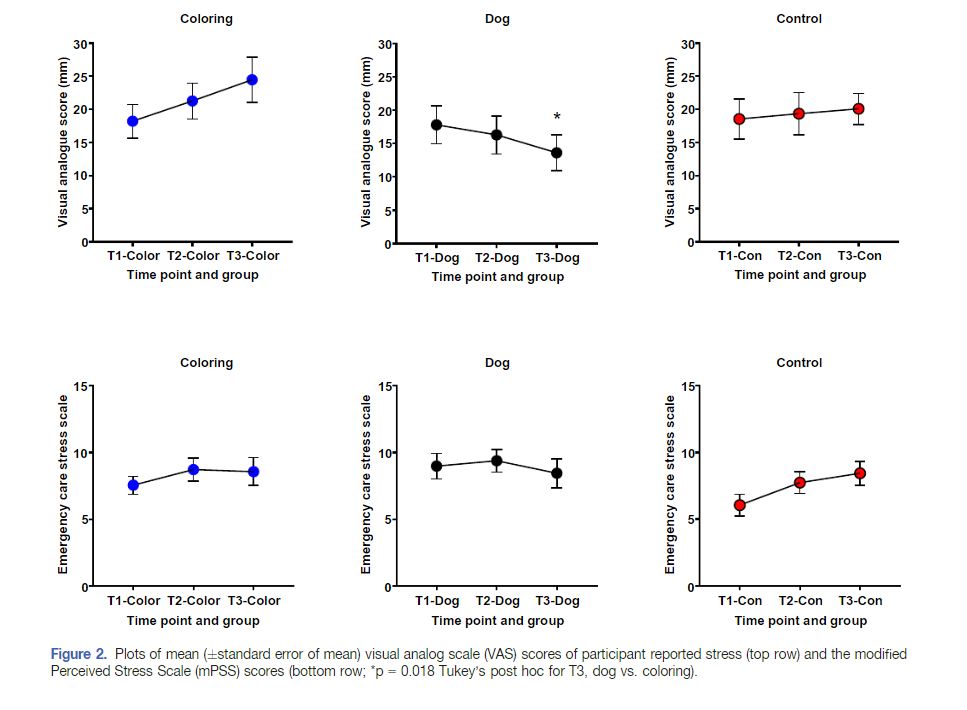
There were two primary outcomes. The first was a self-assessment of stress using a visual analogue scale. The second was a 10-item validated perceived stress scores, altered to focus providers on the past several hours rather than months, as it is originally designed. These were both measured at the beginning of the shift, about 30 minutes after the intervention, and near the end of the shift.
The Results
They enrolled 127 providers, but five withdrew because they thought their shift was too busy to participate. 47% were resident physicians, 23% were attending physicians, and 30% were nurses.
The coloring intervention took a median of five minutes and 26 seconds. In the dog group, providers spent a median of five minutes and 49 seconds with the dogs and had significant interaction with both the dog and the dog’s handler.
Self-reported stress based on the visual analogue scale appears to decrease in the dog therapy group, while it remained level or increased in the art therapy and control groups. However, the only statistically significant change seen using the validated stress scale was an increase in stress from the beginning to the end of the shift in the control group. Salivary cortisol levels (a secondary outcome) were lower at the end of the shift in both intervention groups than the control group.
My thoughts
This is not the kind of study you expect to find when leafing through an academic journal. It is brilliant in its goals and its creativity. Overall, I think it is a well designed study, considering the difficulties inherent in running a trial with therapy dogs and busy emergency clinicians. Of course, no study is without limitations.
We do a full critical appraisal on the SGEM podcast. I would suggest listening to that podcast, because the lead author (Dr. Jeff Kline) provides some very insightful comments explaining why the study was designed as it was. For example, the decision not to randomize people to a control group, based on the concept of “nocebo”, is really interesting. Jeff argues (I think correctly) that if you anticipated being able to see a dog, and instead you were randomized to sit in an empty room by yourself, it might feel like punishment, increasing overall anxiety. Had the authors constructed their study with a group randomized to control, it might have increased the chance of seeing a difference between the dog therapy and control groups. However, it would be harder to know if that difference represented a benefit from the dogs or a harm from the nocebo effect.
The other big limitation of the study is probably the primary outcomes (and I still think there really should only be 1 primary outcome). The amount of stress experienced during a shift is an important outcome, but it is not the most important outcome. If we were going to invest in dog therapy programs (I really liked Ken’s idea of buying every new resident a puppy at the start of their residency), we would really want to see long term reductions in stress and improvement in overall well-being, although that might be a lot to ask from a short intervention on shift.
We clearly need to be creating interventions to reduce stress among emergency providers. However, there are always potential unintended consequences, and we should always consider and measure potential harms. For example, I am incredibly allergic to dogs. I could have self excluded myself from this study, but I also happen to love dogs, and so it is very unlikely that I would have done so. However, I might come to regret the 5 minutes of joy as I spend the rest of my shift significantly distracted by my itchy eyes and fire hydrant of a nose.
I personally dislike colouring, but the first option definitely made me smile, and probably would have cheered me up on a difficult shift. However, if these resources were to find their way into patient care areas, patients might misunderstand the meaning of or be offended by this stress relieving tool.
On a more serious note, harms are possible even with the best intentions. The interventions here took place in a room with no electronic devices, telephone, or window. When I find time to take breaks at work, I prefer to take a few minutes outside to breathe fresh air and hopefully catch some sun. (This was much easier to accomplish in New Zealand than it is in Canada). Barring that, taking a few minutes to check in with my family is very rejuvenating. If I was forced to spend the only 5 minutes I had free during a shift in a room with no windows and no telephone, the presence of colouring pencils would certainly not be enough to override my disappointment.
Bottom line
Although one primary outcome showed a statistical improvement in stress, this study does not convincingly prove a benefit. However, novel approaches to managing stress and burnout are welcomed in emergency medicine. If you like dogs, by all means, maximize the joy in your life by playing with a dog whenever you get the chance. If you like art, take a break to colour. If you like neither, make sure you take some time to do something to reduce the stress of emergency work. You need to look after yourself in order to be able to look after patients.
References
Barker SB, Dawson KS. The effects of animal-assisted therapy on anxiety ratings of hospitalized psychiatric patients. Psychiatr Serv 1998;49(6):797–801.
Bellolio MF, Cabrera D, Sadosty AT, et al. Compassion fatigue is similar in emergency medicine residents compared to other medical and surgical specialties. West J Emerg Med 2014;15(6):629–35.
Bragard I, Dupuis G, Fleet R. Quality of work life, burnout, and stress in emergency department physicians: a qualitative review. Eur J Emerg Med 2015;22(4):227–34.
Kline JA, VanRyzin K, Davis JC, et al. Randomized Trial of Therapy Dogs Versus Deliberative Coloring (Art Therapy) to Reduce Stress in Emergency Medicine Providers [published online ahead of print, 2020 Apr 7]. Acad Emerg Med. 2020;10.1111/acem.13939. doi:10.1111/acem.13939 PMID: 32266765 [article]
Li H, Cheng B, Zhu XP. Quantification of burnout in emergency nurses: A systematic review and meta-analysis. Int Emerg Nurs 2018;39:46–54.
Lu DW, Dresden S, McCloskey C, Branzetti J, Gisondi MA. Impact of Burnout on Self-Reported Patient Care Among Emergency Physicians. West J Emerg Med 2015;16(7):996–1001.
Lundqvist M, Carlsson P, Sjödahl R, Theodorsson E, Levin L-Å. Patient benefit of dog-assisted interventions in health care: a systematic review. BMC Complement Altern Med 2017;17(1):358.
Morgenstern, J. Dog therapy for ED stress?, First10EM, April 13, 2020. Available at:
https://doi.org/10.51684/FIRS.17828


2 thoughts on “Dog therapy for ED stress?”
were the dogs asked how their shift was?
Who let the dogs out? https://www.youtube.com/watch?v=Qkuu0Lwb5EM