
Morgenstern, J. What is the best pad position for cardioversion?, First10EM, April 11, 2022. Available at:
https://doi.org/10.51684/FIRS.127075
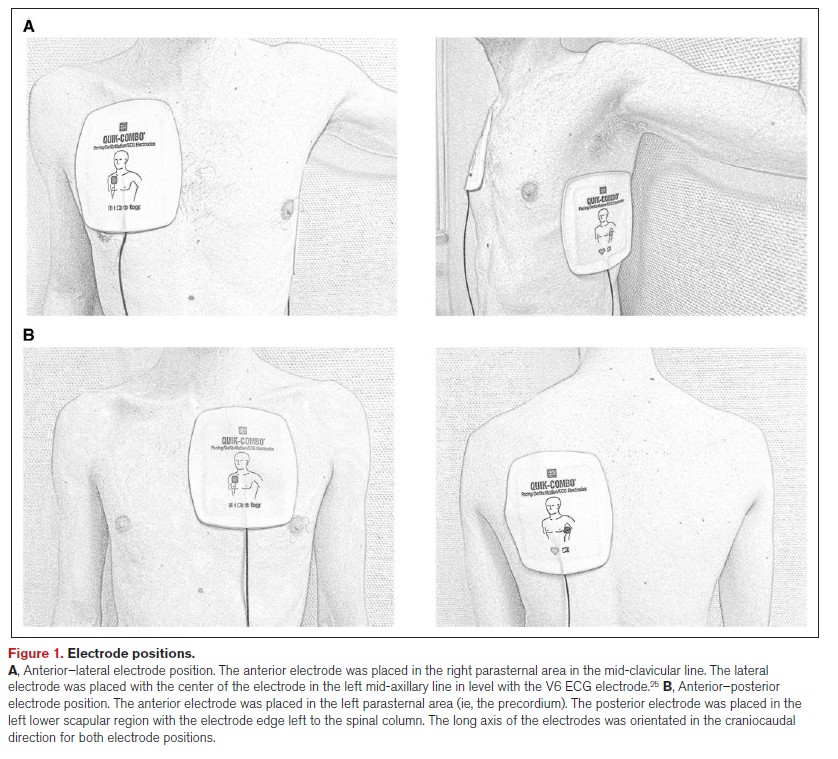
How do you position the pads for cardioversion? Since my time in residency, the AP or anterior-posterior position has largely been favoured. If you had asked me to guess, I might have said that a well done RCT would show that there isn’t much difference. However, this new RCT appears to show a pretty big increase in success with anterior-lateral positioning.
The paper
Schmidt AS, Lauridsen KG, Møller DS, Christensen PD, Dodt KK, Rickers H, Løfgren B, Albertsen AE. Anterior-Lateral Versus Anterior-Posterior Electrode Position for Cardioverting Atrial Fibrillation. Circulation. 2021 Dec 21;144(25):1995-2003. doi: 10.1161/CIRCULATIONAHA.121.056301. Epub 2021 Nov 24. PMID: 34814700 NCT03817372
The Methods
This was a multicenter, open-label, RCT from 3 hospitals in Denmark.
Patients
Adult patients with atrial fibrillation scheduled for elective cardioversion. (These were not emergency patients).
Exclusions: arrhythmias other than AF; implantable devices; hemodynamically unstable AF; untreated hyperthyroidism; known or suspected pregnancy; and those previously enrolled in the trial.
Intervention
Cardioversion using anterior-lateral pad position.
Comparison
Cardioversion using anterior-posterior pad position.
In both groups, a maximum of 4 shocks was administered. They used a strategy of escalating energy, from 100 J, to 150 J, to 200 J, then 360 J.
Outcome
The primary outcome was the proportion of patients in sinus rhythm 1 minute after the first shock.
The Results
They enrolled 468 patients, with just a handful of protocol violations. The mean age was 69, 33% were female, and the mean BMI was 29. About 55% had a prior episode of atrial fibrillation, and 80% were in permanent atrial fibrillation (as opposed to paroxysmal). The median number of days of the current atrial fibrillation episode was about 30.
For the primary outcome, anterior-lateral pad position was significantly better than anterior-posterior after the first shock. Success rate was 54% with anterior-lateral as compared to 33% with anterior-posterior, an absolute difference of 21% (95% CI 13-30%), and a number needed to treat of only 5.
For what I think is the more important outcome, overall success rate, anterior-lateral was still better, with a success rate of 93% as compared to 85% with anterior-posterior (ARR 7%, 95%CI 2-12%, NNT 14).
My thoughts
By far, the biggest problem with this trial is that it was unblinded. They state that this was necessary, given the nature of the study. It was certainty easier to perform this study unblinded, but I don’t think it was strictly necessary. I can easily imagine a setup where patients had 4 pads applied to their chest, and the wires were run through a closed box, such that no one in the room would know which set of pads was live. Although somewhat more expensive, it would have been a much better study design scientifically speaking. That being said, return to sinus rhythm is a relatively objective outcome, and they seems to have standardized other aspects of care (such as the energy delivered and the type and dose of sedation), which will limit bias. On the other hand, an unblinded trial will always be at higher risk of bias that a blinded trial, so we cannot count these results as definitive.
I don’t think their choice of primary outcome is ideal. When making the decision to cardiovert, what we care about is overall success. Whether that happens the first time we hit the button or the third is rather inconsequential. This is especially true in this study, when they chose to use progressively increasing doses for each shock. That means that the first two shocks were probably at an inadequate dose, and so basing the primary outcome on those shocks seems silly. I always go straight to 200 joules, and I believe there is good data that doing so actually decreases the total energy that the average patient receives, because fewer total shocks are required.
These were not emergency department patients. The median duration of this episode of atrial fibrillation was 30 days. Only 20% had the diagnosis of paroxysmal afib, with the other 80% having the diagnosis of permanent atrial fibrillation. I don’t think the chronicity will impact whether AP or AL pad placement is better. However, persistent atrial fibrillation tends to be much more shock resistant. Therefore, our success rates might be much higher in the emergency department, and if success rates are higher, the difference between the groups might end up a lot smaller.
It is a minor point that will only stand out to some of my nerdiest readers, but I find it very odd that the very first statement in their methods section is, “the data, analytic methods, and study materials will not be made available to other researchers for the purposes of reproducing the results or replicating the procedure.” Data sharing and replication are core to the scientific process. Every statement on good scientific practice I have read states that data sharing is essential. It is common for researchers to refuse to share their data, but I found it surprising for them to state their refusal so bluntly.
Finally, it is worth noting that there are two prior RCTs looking at this same question. Walsh (2005) looked at 307 patients with atrial fibrillation. The results were statistically insignificant, although the point estimates were similar to those in this study (95% success after 4 shocks in anterior-lateral as compared to 88% with anterior-posterior). Brazdzionyte (2006) is another RCT in 103 elective atrial fibrillation patients, and there were no differences at all (with only 1 failure in both groups).
Bottom line
The unblinded nature of this trial leaves room for bias, and it may not translate perfectly to emergency department patients, but there is a big enough difference to be clinically important, so I think it makes sense to perform cardioversions for atrial fibrillation using the anterior-lateral pad position until we see better evidence.
References
Brazdzionyte J, Babarskiene RM, Stanaitiene G. Anterior-posterior versus anterior-lateral electrode position for biphasic cardioversion of atrial fibrillation. Medicina (Kaunas). 2006;42(12):994-8. PMID: 17211107
Schmidt AS, Lauridsen KG, Møller DS, Christensen PD, Dodt KK, Rickers H, Løfgren B, Albertsen AE. Anterior-Lateral Versus Anterior-Posterior Electrode Position for Cardioverting Atrial Fibrillation. Circulation. 2021 Dec 21;144(25):1995-2003. doi: 10.1161/CIRCULATIONAHA.121.056301. Epub 2021 Nov 24. PMID: 34814700
Walsh SJ, McCarty D, McClelland AJ, Owens CG, Trouton TG, Harbinson MT, O’Mullan S, McAllister A, McClements BM, Stevenson M, Dalzell GW, Adgey AA. Impedance compensated biphasic waveforms for transthoracic cardioversion of atrial fibrillation: a multi-centre comparison of antero-apical and antero-posterior pad positions. Eur Heart J. 2005 Jul;26(13):1298-302. doi: 10.1093/eurheartj/ehi196. Epub 2005 Apr 11. PMID: 15824079


2 thoughts on “What is the best pad position for cardioversion?”
Maybe I am doing it wrong but for my AP placement, I leave the anterior pad more Rt sternal border (than Lt sternal border). My image of where the heart is located within the chest and possibly flawed concept of the vector of the current will give a greater vector of current though more of the heart than placing the anterior pad on the Lt sternal border which I think may miss the more of mass of the heart if the heart is located more centrally.
I tend to agree. Although, I was surprised by these results, as based on that same logic, I would have thought that AP would be better, which it clearly wasn’t here.