Morgenstern, J. Steroids for pneumonia (CAPE COD and ESCAPe), First10EM, April 24, 2023. Available at:
https://doi.org/10.51684/FIRS.129950
I’ve gone in depth into the topic of steroids for pneumonia previously. (Also covered on the EM Cases Journal Jam.) At the time, despite some promising point estimates, I thought that the evidence was too weak to suggest regular use of steroids for community acquired pneumonia. In that write up, I did mention a number of major trials that had been registered, and the largest of those – the CAPE COD trial – has just been published with fairly impressive results. However, the ESCAPe trial was also published, and perhaps because it was a negative trial, received far less fanfare. This post will look at both trials.
Paper 1: CAPE COD
CAPE COD: Dequin PF, Meziani F, Quenot JP, Kamel T, et al. Hydrocortisone in Severe Community-Acquired Pneumonia. N Engl J Med. 2023 Mar 21. doi: 10.1056/NEJMoa2215145. Epub ahead of print. PMID: 36942789 [NCT02517489]
The Methods
A multicentre, double-blind, placebo controlled RCT from 31 ICUs in France.
Patients
Adult patients being admitted to the ICU with severe community acquired pneumonia.
Severe was defined as mechanical ventilation with PEEP of at least 5 cm water, an PaO2:FiO2 ratio estimated to be less than 300, or a Pulmonary Severity Index score of more than 130.
Exclusions: Pneumonia caused by influenza, septic shock, history suggestive of aspiration, baseline steroid use equivalent to 15mg of prednisone or more daily, active tuberculosis or fungal infection.
Intervention
Hydrocortisone, given as a continuous infusion of 200 mg/day intravenously, with a planned taper, for a total of either 8 or 14 days depending on whether the patient was improving on day 4.
Comparison
Placebo (intravenous saline using the same protocol).
Outcome
The primary outcome was 28 day all cause mortality.
The Results
Of a planned 1200 patients, they enrolled 800. Because of a few other exclusions, the final study cohort is 795. The trial was stopped early, primarily because of COVID.
There was a significant decrease in mortality (the primary outcome), with 6.2% of the hydrocortisone group and 11.9% of the placebo group being dead at 28 days (ARR 5.6%, 95% CI -9.6 to -1.7%, p=0.006).
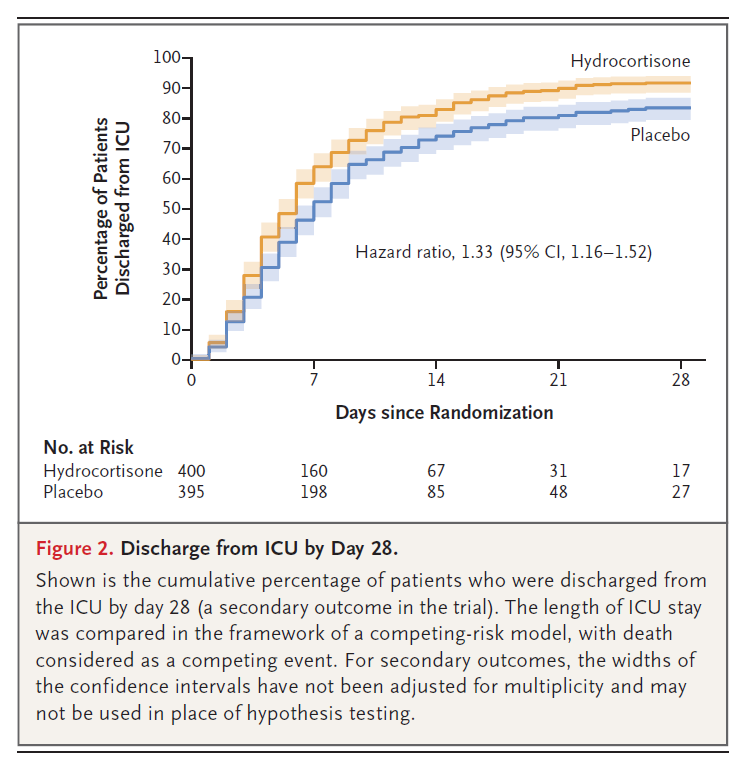
About half the group weren’t on mechanical ventilation at the time of enrollment, and subsequent intubation was also lower in the steroid group (18% vs 30%).
There were no obvious differences in the safety outcomes of GI bleed, ventilator-associated pneumonia, or bloodstream infections. Sugars were higher in the steroid group, with a significantly higher daily insulin dose.
My thoughts on CAPE COD
This is a good study, with strong methodology, using an important primary outcome.
It was stopped early, and the mortality was lower than expected, which adds some uncertainty. Trials stopped early tend to overestimate benefits, and that would make sense to me, as almost no treatments decrease mortality by 6%.
With less than 15% of screened patients being enrolled, selection bias is a concern, and generalizability is limited. If you find yourself giving steroids to 100% of pneumonia patients after the publication of this study, you probably aren’t following the inclusion and exclusion criteria of these studies.
The exclusion of influenza might be important, because the current best evidence (which is very weak) suggests harm from steroids in influenza. I imagine all ICU patients are getting viral testing these days, but that isn’t true of all pneumonia patients. Most importantly, this exclusion will mean that emergency physicians should not be rushing to start treatment until all test results are back.
The biggest worry after this trial will be indication creep. We know steroids cause harm. This trial looked at a very specific group of patients with well defined pneumonia and clear markers of severity. They excluded septic shock. They excluded aspiration pneumonia. They excluded influenza, post-obstructive pneumonia, and cystic fibrosis, among a much longer list. There is a big risk that as this practice is adopted in the real world, it will be applied more liberally, and that in a less carefully selected population the harms might more evenly balance the benefits.
Both of the trials discussed today provide steroids as an infusion. Although there are some theoretical reasons this might be a good idea (fewer swings in blood glucose), it isn’t clear that infusions are better than intermittent dosing, and the practical problems with running infusions in sick patients could cause problems. I think infusions are reasonable once patients are settled in the ICU, but for emergency department management, I imagine I will just provide a single bolus once I determine that the patient fits criteria for treatment.
PAPER 2: ESCAPe
Meduri GU, Shih MC, Bridges L, Martin TJ, El-Solh A, et al. Low-dose methylprednisolone treatment in critically ill patients with severe community-acquired pneumonia. Intensive Care Med. 2022 Aug;48(8):1009-1023. doi: 10.1007/s00134-022-06684-3. Epub 2022 May 13. PMID: 35723686 [NCT01283009]
The Methods
A multicentre, double-blind, placebo controlled RCT from 42 American hospitals.
Patients
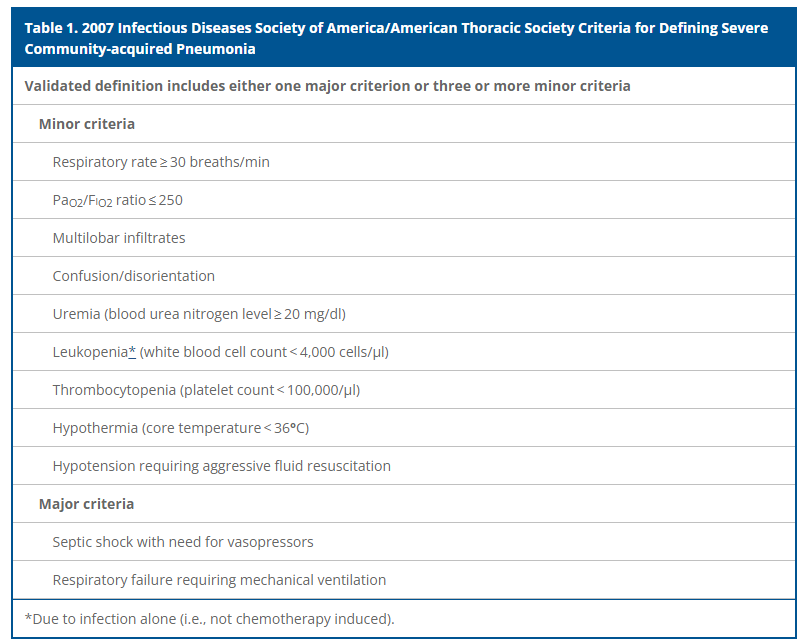
Adult patients with severe community acquired pneumonia being admitted to the ICU. (Severity based on the IDSA/ATS criteria, as below.)
Intervention
Methylprednisolone infusion for 20 days. (40 mg loading dose, then 40 mg/day on days 1–7, 20 mg/day on days 8–14, 12 mg/day on days 15–17 and 4 mg/day on days 18–20). At the time of ICU discharge patients were switched from an infusion to twice a day dosing.
Comparison
Matching placebo.
Outcome
The primary outcome was all cause mortality at 60 days.
The Results
They screened 3936 patients, and enrolled 584. Recruitment was much slower than anticipated. The study was powered for 1406 patients, and it was stopped early, not because it reached any specific stopping point, but just because they hit their planned end date.
The mean age was 69 years, 96% were male, and 83% were white. (This was in the Veterans hospital system in the United States.) 33% of patients were on mechanical ventilation at the time of enrollment.
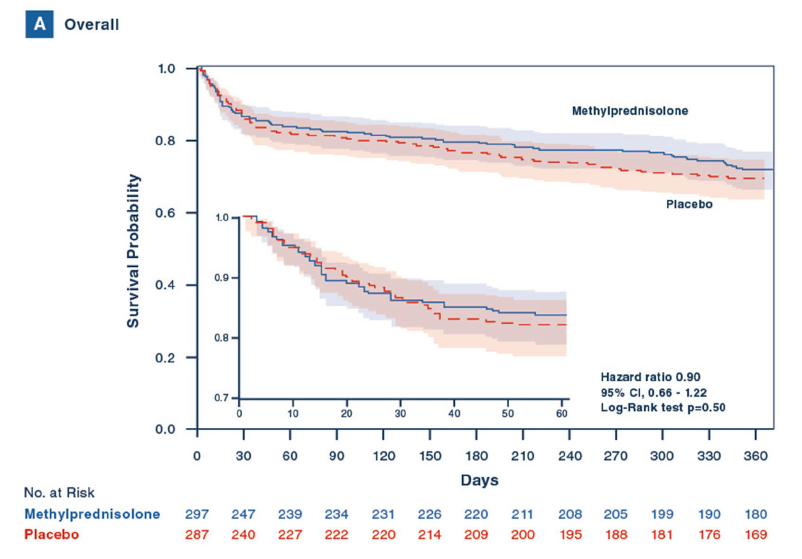
For the primary outcome, there was no difference in mortality (16% vs 18%, ARR-2%, 95% CI -8 to 5%, p=0.61). Mortality was also similar at 180 days.
There were no differences in the secondary outcomes, including vasopressor-dependent shock, ARDS, days of mechanical ventilation, ICU length of stay, or hospital length of stay. Adverse events were also not statistically different.
My thoughts on ESCAPe
This is another very high quality study, with excellent methodology, but also with the problem of being stopped without hitting the desired sample size.
Being from the VA hospital system in the United States, this is almost entirely males. I have never seen anything to make me think that steroids would have different outcomes based on biologic sex, but there is a lot we don’t know about the impacts of sex in medicine, because females have long been underrepresented in medical research.
A brief comment on publication bias: ESCAPe was finished in 2016, and so took 6 years to get published. CAPE COD stopped enrollment in July 2021, and so took just over 1.5 years to get published. Despite being equally good and equally important papers, the positive paper is published much faster, in a bigger journal, and publicized far more. (The FOAMed community is at least partially responsible for the disproportionate emphasis placed on CAPE COD.)
Bottom line
Both CAPE COD and ESCAPe are high quality trials. The results are somewhat conflicting, and we should be cautious about over-emphasizing the positive result over the negative result. That being said, overall mortality was 2% lower in the steroid group in ESCAPe, and the trial ended up being significantly underpowered. I think the best current guess is that there is a small mortality benefit of steroids in patients with severe community acquired pneumonia in the ICU. (My guess is it will be closer to the 2% of ESCAPe than the 6% of CAPE COD.) With mixed results, we should be very cautious about being too definitive in our conclusions. This should remain an area of active research. Clinically speaking, I will provide steroids to the select group of ICU patients with community acquired pneumonia who don’t have contra-indications to steroids, but I will be very cautious to guard against indication creep, because we know steroids have many significant complications.
Other FOAMed
PulmCrit Hot Take: Steroid for severe pneumonia (CAPE COD trial)
Steroids for community acquired pneumonia – the evidence
Journal Jam 17 – Steroids for CAP and COVID Pneumonia
FOAM Cast: Steroids for Severe Community-Acquired Pneumonia
References
Dequin PF, Meziani F, Quenot JP, Kamel T, Ricard JD, Badie J, Reignier J, Heming N, Plantefève G, Souweine B, Voiriot G, Colin G, Frat JP, Mira JP, Barbarot N, François B, Louis G, Gibot S, Guitton C, Giacardi C, Hraiech S, Vimeux S, L’Her E, Faure H, Herbrecht JE, Bouisse C, Joret A, Terzi N, Gacouin A, Quentin C, Jourdain M, Leclerc M, Coffre C, Bourgoin H, Lengellé C, Caille-Fénérol C, Giraudeau B, Le Gouge A; CRICS-TriGGERSep Network. Hydrocortisone in Severe Community-Acquired Pneumonia. N Engl J Med. 2023 Mar 21. doi: 10.1056/NEJMoa2215145. Epub ahead of print. PMID: 36942789
Meduri GU, Shih MC, Bridges L, Martin TJ, El-Solh A, Seam N, Davis-Karim A, Umberger R, Anzueto A, Sriram P, Lan C, Restrepo MI, Guardiola JJ, Buck T, Johnson DP, Suffredini A, Bell WA, Lin J, Zhao L, Uyeda L, Nielsen L, Huang GD; ESCAPe Study Group. Low-dose methylprednisolone treatment in critically ill patients with severe community-acquired pneumonia. Intensive Care Med. 2022 Aug;48(8):1009-1023. doi: 10.1007/s00134-022-06684-3. Epub 2022 May 13. PMID: 35723686



3 thoughts on “Steroids for pneumonia (CAPE COD and ESCAPe)”
I think one interesting fact in the Cape Cod trial was that they included Asthmatics and also COPD pt’s in their cohorts, I wonder if withholding steroids in these pt’s resulted in the increase in mortality in the placebo group?