Morgenstern, J. Paxlovid doesn’t work for long COVID either (The STOP-PASC trial), First10EM, June 10, 2024. Available at:
https://doi.org/10.51684/FIRS.136731
As we have covered multiple times before, the evidence for paxlovid is heavily conflicted and mostly negative. There is very little reason to be using this agent clinically. However, despite an utter lack of evidence, many people have held out hope that paxlovid might be the miracle cure for the nebulous long COVID syndrome (referred to here as postacute sequelae of SARS-CoV-2 infection). The first trial has now been published, and the results are completely unsurprising.
The paper
STOP-PASC: Geng LN, Bonilla H, Hedlin H, et al. Nirmatrelvir-Ritonavir and Symptoms in Adults With Postacute Sequelae of SARS-CoV-2 Infection: The STOP-PASC Randomized Clinical Trial. JAMA Intern Med. 2024 Jun 7:e242007. doi: 10.1001/jamainternmed.2024.2007. PMID: 38848477 NCT05576662
The Methods
This is a single center double-blind RCT from the outpatient setting at 1 American University looking at the use of paxlovid for long COVID symptoms.
Patients
Adult patients over 40 kg, with an eGFR over 60mL/min, with a confirmed COVID-19 infection more than 90 days prior to enrollment, and persistent postacute sequelae of SARS-CoV-2 infection symptoms as determined by a physician. Patients had to have “at least 2 self-reported moderate or severe core symptoms or symptom clusters defined as fatigue, brain fog,body aches, cardiovascular symptoms,shortness of breath, and gastrointestinal symptoms.”
Exclusions: Pregnancy, breast-feeding, severe liver disease, active SARS-COV-2 infection, use of any SARS-CoV-2 treatment within 30 days, COVID vaccination within 30 days, medication interactions.
Intervention
Paxlovid (nirmatrelvir, 300mg, with ritonavir, 100mg) BID for 15 days.
Comparison
The control was a matching placebo with 100 mg of ritonavir, also BID for 15 days.
Outcome
The primary outcome was core symptom severity over the previous 7 days when asked at 10 weeks.
The Results
They screened 784 patients, 168 were eligible, and 155 were ultimately randomized. They were supposed to enroll 200, but the trial was stopped early for futility.
There was no difference in the primary outcome, core symptom severity at 10 weeks. The actual numbers are somewhat difficult to interpret, but are probably consistent with randomness (some symptoms were better and some worse). There seem to be mathematical errors in their results, such as the proportion of weeks with fatigue being 0.15 in both groups, but that somehow being statistically different with a p value of 0.02.
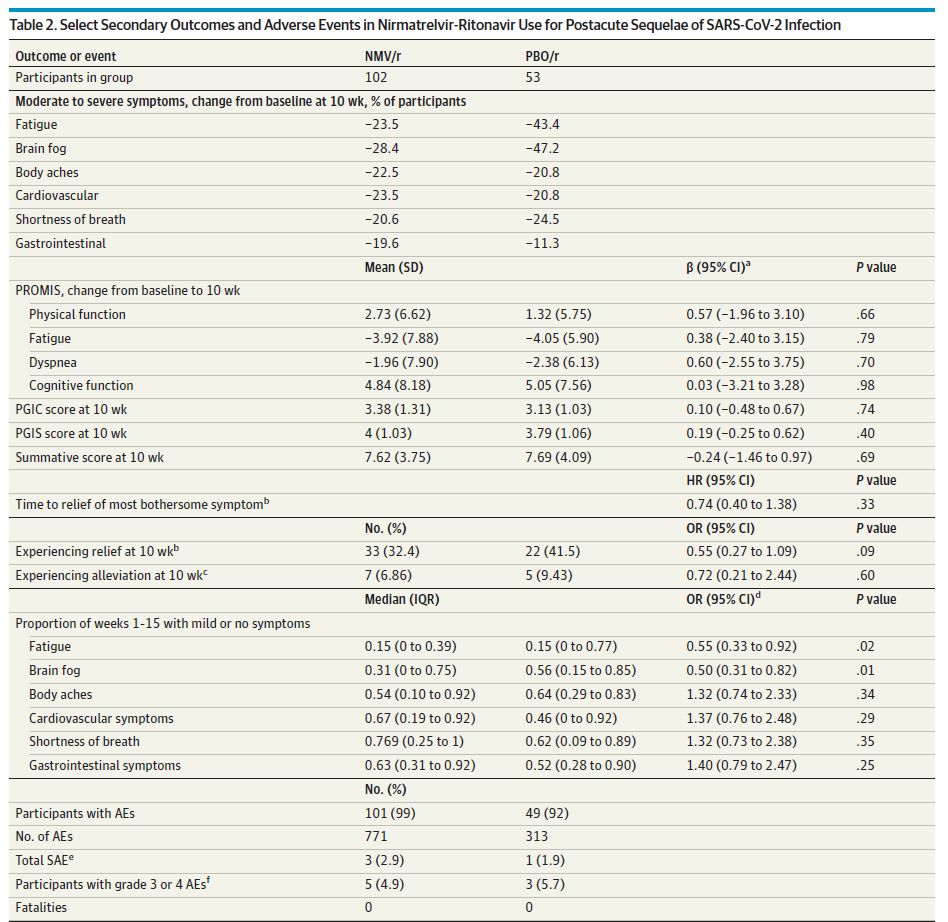
There is not a difference in adverse events, but the definition they used meant that 99% of the treatment group and 93% of the placebo group had adverse events. Those numbers are ridiculous, and tell us that their definition was useless. That being said, a 6% absolute increase in adverse events is believable, and clearly harmful if there is not benefit to this medication. (Remember that both groups here received active ritonavir, and so the adverse event rate of a true placebo group would be lower.)
My thoughts
Although we clearly need RCTs on the management of long-COVID symptoms, paxlovid seems like an odd place to start. It is an ‘antiviral’ that doesn’t even work in the acute phase of infection. As far as pre-test probability goes, the idea of using an ‘antiviral’ medication to treat post-viral symptoms is somewhat silly. However, there is a theory (with little evidence) that chronic viral infection is the cause of long-COVID symptoms, and that is the theory that underlies this trial.
Overall, this is a well designed trial. The protocol registered on clinicaltrials.gov matches the final manuscript, which is sadly a rarity.
There are some fundamental problems with this trial that will plague all future long-COVID research. Given that there is no gold-standard definition of long-COVID, the patient population here is somewhat nebulous, and might be difficult to recreate in clinical practice. Furthermore, the symptoms are all vague, subjective, and not necessarily related to the same underlying pathophysiology in all patients. Without a solid understanding of the underlying pathophysiology of these patients’ symptoms, it is going to be hard to determine the best approach to treatment.
Although selection bias is always a concern, the ratio here seems higher than usual, with 784 patients screened for the 168 enrolled. (This might just represent how difficult a drug paxlovid is to prescribe.)
Rather than using a pure placebo, they gave all patients ritonivir (which has no anti-viral activity, but is included to slow nirmatrelvir metabolism). They did this because ritonavir causes the well known paxlovid side effect of dysgeusia, and therefore the inclusion makes it less likely the the groups will become unblinded. This is an important consideration for their subjective primary outcome, and I think it was the right way to run the trial. However, it means that the side effects of the placebo group are dramatically over-estimated, and therefore the harms of treatment are dramatically under-estimated.
Ultimately, these results are not at all surprising. Paxlovid doesn’t even seem to work when given early in the midst of acute viral replication, so giving it to patients with vague symptoms of undetermined etiology does not make a lot of sense.
Bottom line
This is the first RCT of paxlovid for long-COVID, and it is very clear that it should not be prescribed for this indication (nor for almost any indication) at this time.
Other FOAMed
EPIC-SR: The negative paxlovid data Pfizer has been sitting on
EPIC-HR: Some underwhelming data on Paxlovid
Paxlovid evidence: still very little reason to prescribe
Evidence based medicine is easy
Evidence based medicine resources
References
STOP-PASC: Geng LN, Bonilla H, Hedlin H, et al. Nirmatrelvir-Ritonavir and Symptoms in Adults With Postacute Sequelae of SARS-CoV-2 Infection: The STOP-PASC Randomized Clinical Trial. JAMA Intern Med. 2024 Jun 7:e242007. doi: 10.1001/jamainternmed.2024.2007. PMID: 38848477