


Some big and potentially practice changing articles this month. (I tend to read ridiculous articles in my free time, which I have had very little of, and so there are no intubation in outer space or highly philosophical papers about the language this month. Don’t worry, there is still a very bad joke.)
BiPAP for preoxygenation could be a big game changer
Gibbs KW, Semler MW, Driver BE, Seitz KP, et al. Noninvasive Ventilation for Preoxygenation during Emergency Intubation. N Engl J Med. 2024 Jun 13. doi: 10.1056/NEJMoa2313680. PMID: 38869091
I think this trial is probably practice changing, at least for many people. Are you using the best technique for preoxygenation? This multicenter RCT randomized 1301 critically ill adult patients in the ED or ICU to either facemask oxygen or BiPAP for their 3 minute preoxygenation. For their primary outcome of desaturation to less than 85%, BiPAP was significantly better, with 19% of the face mask group desaturating and only 9% of the BiPAP group. This is an important outcome, but it is a surrogate outcome. Peri-intubation cardiac arrest was an exploratory secondary outcome, and also looked better with BiPAP (1.1% vs 0.2%). This is an unblinded trial, and oxygen saturation is not perfectly objective. However, despite being an imperfect trial, I think the pretest probability is high enough that this should probably change practice. (As compared to drugs, which rarely work and have many side effects, we know BiPAP, or specifically PEEP, is important in treating hypoxia, with very few downsides.) Admittedly, I am biased, because this trial agrees with my current practice. If you have heard my “RSI and then they die” talk, you will know I am a big supporter of first identifying shunt, and then aggressively treating it with PEEP in the preoxygenation period, and that I think BiPAP or NIPPV is probably the best overall approach to providing PEEP in the pre-intubation resuscitation period. The big remaining question is how widespread this practice should become. My sense is that most patients don’t need BiPAP. If a patient is satting 100% on flush rate oxygen, I don’t think this technique is necessary. (Although in hemodynamically unstable patients, I do like to trial positive pressure ventilation before intubating to get a sense of its impacts on hemodynamics.) However, If I can’t get the sats above 95% on a nonrebreather in a patient who is breathing with an open airway, I know there is some degree of shunt, and adding PEEP with NIPPV makes a lot of sense.
I go into more details on this paper in the main blog post.
Bottom line: This unblinded multicenter RCT demonstrates a decrease in peri-intubation hypoxia (and potentially cardiac arrest) from the use of BiPAP for preoxygenation. This is a technique all emergency doctors should be using on a significant proportion of their patients, even if it isn’t needed routinely.
Scott Weingart disagrees with my conclusion, and thinks that noninvasive or PEEP of some sort should now routinely be used as part of a standard operating procedure for all emergency department and critically ill patients. A big part of his argument is that the positive effects hold true among all subgroups, even among patients who were on room air before intubation, and therefore are unlikely to have shunt physiology. He points to some evidence that patients with damaged lungs quickly develop atelectasis, even within the 1 minute apneic period of RSI, which would explain the benefit seen. Worth considering, and I look forward to hearing other perspectives.
Andexanet is expensive and harmful (so try to ignore the drug company sales pitch, even if it’s published in the New England Journal)
Connolly SJ, Sharma M, Cohen AT, et al. Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage. N Engl J Med. 2024 May 16;390(19):1745-1755. doi: 10.1056/NEJMoa2313040. PMID: 38749032
Although my hospital has been spending ridiculous amounts of money to stock this drug, there is absolutely no evidence it helps our patients. They managed to move a lot of product based on a previous completely uncontrolled observational cohort, which is a pretty sad comment on the state of evidence based medicine. We finally have our first RCT, and it is going to be important to move beyond the conclusion written by the drug company. (Actually the entire paper was written by the drug company, and the trial was entirely designed and run by the drug company. That we allow such crazy financial conflicts of interest in medical science remains a massive ongoing problem.) This is an unblinded multicenter trial in which 550 patients with intracranial hemorrhage who had taken one of apixaban, rivaroxaban, or edoxaban within 18 hours were randomized to andexanet or usual care (which was mostly 4 factor PCC). Their surrogate outcome of ‘hemostatic efficacy’ was improved with andexanet (67% vs 53%), but the only thing that really changed was hematoma size, and their own data basically proves that surrogate outcome was pointless. All of the clinical outcomes were identical or worse with andexanet. Neurologic outcomes were the same. There was a significant increase in thrombotic events, including an increase in ischemic strokes. MI and death were statistically the same, but both were numerically worse in the andexanet group. This is an unblinded trial, at high risk of bias, completely run by the drug company, and still manages to show worse clinical outcomes with andexanet. It is about as big a nail you can get for a very small coffin. Andexanet clearly should not be used, and hospitals should stop wasting money on this unproven drug.
Bottom line: This is the first RCT of andexanet for Xa inhibitor reversal, and despite the surrogate outcome the drug company wants you to focus on, all of the clinical outcomes were worse with treatment. Andexanet has no clinical role in mid 2024.
Aslanger: Another STEMI-equivalent pattern to learn
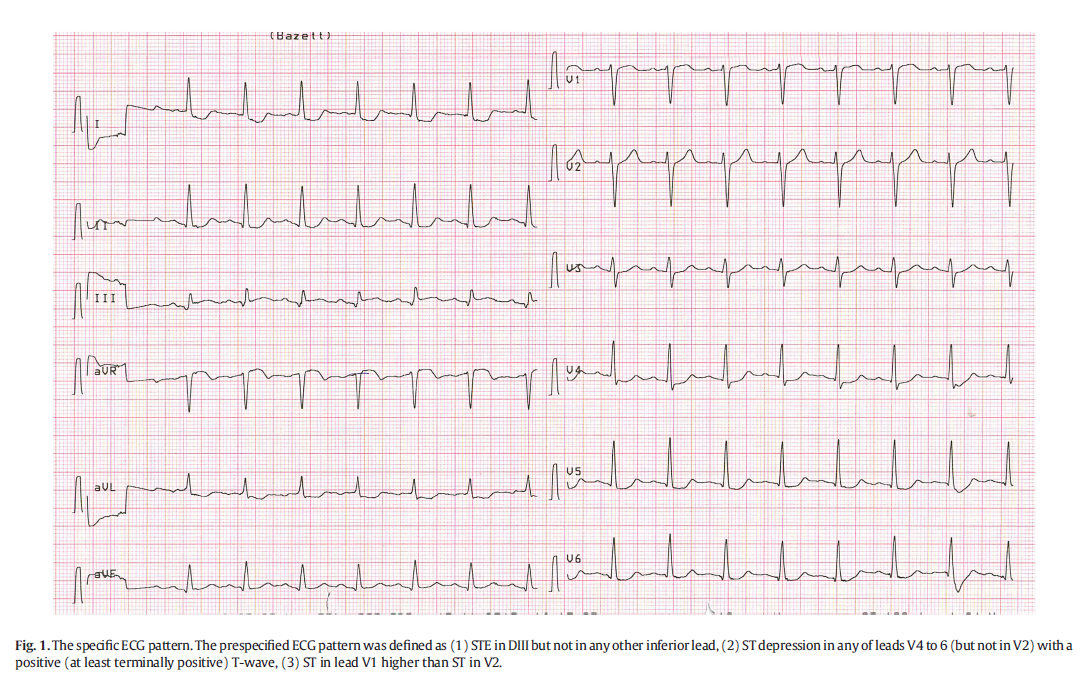
Aslanger E, Yıldırımtürk Ö, Şimşek B, Sungur A, Türer Cabbar A, Bozbeyoğlu E, Karabay CY, Smith SW, Değertekin M. A new electrocardiographic pattern indicating inferior myocardial infarction. J Electrocardiol. 2020 Jul-Aug;61:41-46. doi: 10.1016/j.jelectrocard.2020.04.008. Epub 2020 Apr 13. PMID: 32526537
By now, we all know that there is more to STEMI than ST elevation. There are numerous accepted STEMI-equivalent ECG patterns, and this paper described a new one that we should probably know. (Relatively new, as this was published in 2020.) With inferior STEMI, there is a subset where the vector shifts somewhat to the right, to about 90 degrees with aVF, resulting in a pattern consistent with inferior occlusive MI, with these ECG characteristics: “any STE in DIII but not in other inferior leads, (2) STD in any of leads V4 to V6 (but not in V2) with a positive or terminally positive T-wave, (3) ST in lead V1 higher than ST in V2”. In this retrospective study, they looked at 1000 patients diagnosed with “NSTEMI” and retrospectively looked at their ECGs. 6.3% of the NSTEMI group had this pattern. This subset had worse outcomes than the average NSTEMI group, with similar rates of mortality to a control group of patients with formally diagnosed inferior STEMI. The pattern was not perfect for angiographically proven coronary occlusion, but is probably high enough to warrant urgent intervention. 25% of the group had acute occlusion at the time of angiography (as compared to 69% with classic STEMI and 16% of the group with NSTEMI without this pattern.) Of course, this is not a perfect comparison, because these patients were all diagnosed as “NSTEMI”, and so were not getting immediate angiograms like the STEMI groups, and there is a reasonable high rate of spontaneous reperfusion if you are putting these angiograms off until the next day. Based on a surrogate outcome that looks at peak troponin levels among other things, they thought that 54% of these patients had an occluded coronary (as compared to 97% with the classic STEMI pattern). Obviously, this data isn’t perfect, and the numbers fall somewhere between the classic STEMI pattern and NSTEMI, but this group looks to be high enough risk that I will call interventional radiology about all of these patients, quoting the “Aslanger pattern” and the more than 50% risk of coronary occlusion, and get them involved to decide. (I have been looking for this pattern for a while, but only because I am an avid reader of the Dr. Smith ECG blog. See posts here and here for examples.)
Bottom line: Although imperfect, I would learn and watch for this “Aslanger ECG pattern”, as it probably warrants a call to interventional.

Suck at NG tubes like me? This might help
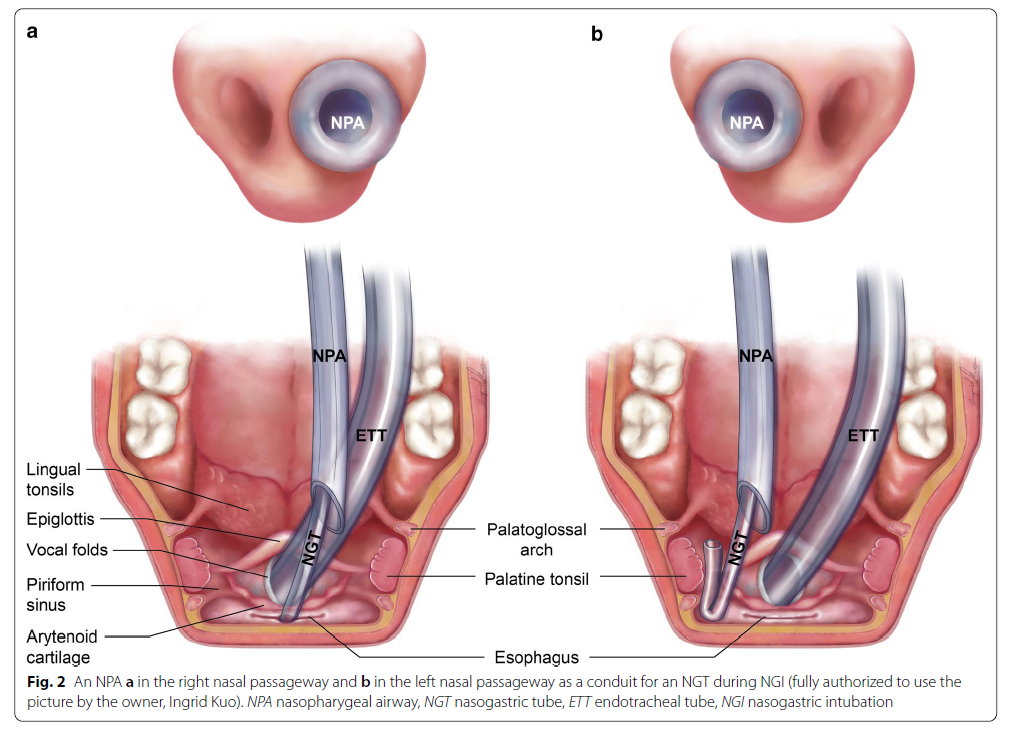
Huang TY, Lin JR, Chung YT. A preinstalled nasopharyngeal airway in the right nasal passageway to facilitate nasogastric intubation in anesthetized and intubated patients: a prospective randomized controlled trial. BMC Gastroenterol. 2020 Nov 3;20(1):365. doi: 10.1186/s12876-020-01514-6. PMID: 33143639 NCT03697642
I love it when people use RCTs to assess seemingly simple interventions, especially when the intervention can address my personal short-comings. I consider myself a reasonably good proceduralist. I love performing LPs. When colleagues are struggling or concerned, I will happily jump in to perform just about any procedure required. However, for some reason the NG tube, despite being such a simple and common procedure, is one I have never been able to master. This is a simple RCT looking at adult patients undergoing elective abdominal surgery who ‘required’ an NG tube. They were randomized to either standard care (placing the NG tube directly through the nare) or to have a preinstalled nasopharyngeal airway through which the NG tube was placed. (After NG tube placement, the nasopharyngeal airway was pulled back and cut off.) Unfortunately, the study had 4 primary outcomes, was unblinded, and all procedures were performed by a single very experienced anesthesiologist. Therefore, this is an imperfect study with imperfect generalizability. However, the outcomes were relatively dramatic. Use of the nasopharyngeal airway resulted in a big improvement in first attempt success from 47% to 83% (p<0.001, ARR 35.7%, 95% CI 19-52%). The numbers were a little closer after 2 attempts (89% vs 64%), but still clearly favoured the nasopharyngeal airway. The procedure also took about 30 seconds more with the preloaded nasopharyngeal airway (which doesn’t really make sense, and might indicate some underlying bias, in that this researcher tried harder when the NPA was in place). They only used the right nare, and they provide the image below to explain their logic, but I think I would just rotate the nasal airway if I wanted to use the left nare. This was only in intubated patients, so it is unclear if similar benefits exist in the awake patient, but I think it probably would.
Bottom line: Despite being a low quality single center unblinded RCT, I think this is practice changing for me, and I will use a nasal airway as an introducer for NG tubes from now on.

The methylene blues
Pruna A, Bonaccorso A, Belletti A, Turi S, Di Prima AL, D’amico F, Zangrillo A, Kotani Y, Landoni G. Methylene Blue Reduces Mortality in Critically Ill and Perioperative Patients: A Meta-Analysis of Randomized Trials. J Cardiothorac Vasc Anesth. 2024 Jan;38(1):268-274. doi: 10.1053/j.jvca.2023.09.037. Epub 2023 Oct 1. PMID: 37880041
We tried methylene blue a few times when I was a trainee in the ICU, and the patients always died. With that background, the fact this is more of an ICU than ED intervention, and the fact that I have never seen a high quality study worth discussing, this topic has never really piqued my interest. However, podcast co-host Casey Parker was recently asked by ICU to give methylene blue in the ED, and so we thought we should have a look at the literature. There is a recent meta-analysis of 11 RCTs, which mixed studies of septic shock with post-surgical vasoplegia, encompassing a total of 556 patients. The headline news was a lower mortality with methylene blue (RR 0.6, 95%CI 0.43-0.84). That sounds promising, but obviously a meta-analysis is only as strong as the studies it summarizes. I have not had time (or interest) to read all of the individual RCTs, but I clicked through to 2 of them, and despite claiming to be “placebo” controlled, they used saline, which is clearly nothing like methylene blue, and therefore the trials were clearly not blinded. (Blinding will always be difficult given the multitude of clinical changes after giving methylene blue.) These are mostly studies of less than 50 patients. This is the exact kind of topic and study where you would expect publication bias, where negative studies are never published. The authors claim 0% statistical heterogeneity, but that tells you a lot about how valuable the i squared statistic is, because we are talking about combining completely different clinical populations here, so clinical heterogeneity is very high. Overall, this is a promising hypothesis generator, but not a clinical practice changer. We don’t need any more systematic reviews on the topic (of which there are way more than actual RCTs). What we really need are large, high quality RCTs. Whether you should use this clinically will remain an open debate. I think we probably do more harm than good to critically ill patients when “throwing the kitchen sink at them”, and methylene blue probably fits in that category. However, improved mortality (and at least temporarily improved hemodynamics), even in low quality papers, might justify occasional use in the right patient not responding to traditional vasopressors (which admittedly also don’t have great evidence of patient benefit).
Bottom line: Methylene blue for septic shock remains in the “unproven” category, but there is a systematic review concluding improved survival, so you could start hearing about this more often.
Another swing and a miss for paxlovid
STOP-PASC: Geng LN, Bonilla H, Hedlin H, et al. Nirmatrelvir-Ritonavir and Symptoms in Adults With Postacute Sequelae of SARS-CoV-2 Infection: The STOP-PASC Randomized Clinical Trial. JAMA Intern Med. 2024 Jun 7:e242007. doi: 10.1001/jamainternmed.2024.2007. PMID: 38848477
Long COVID is clearly a problem for many patients, and so it is nice to see RCTs attempting to address that problem. However, using an unproven ‘antiviral’ medication to address symptoms occurring 3 months after a viral infection doesn’t make a lot of sense to me. That’s what they tried to do in the STOP-PASC trial, in which patients with symptoms thought to be from long COVID, at least 90 days after confirmed COVID infection, were randomized to paxlovid or placebo. Unsurprisingly, the trial was stopped early for futility with 155 patients, and there were absolutely no differences between the groups. I believe the main results, because there is almost no reason to think paxlovid would help with long COVID symptoms. They also found no difference in adverse events, but I don’t buy that outcome. They used a definition of adverse events that meant that 99% of the paxlovid group and 93% of the placebo group had an ‘adverse event’. That is clearly a useless definition. The big issue going forward is that we don’t have a gold standard definition of long COVID, there are no clinical markers, and we do not understand the underlying pathophysiology. With those limitations, it is going to be very hard to know who to include in these studies and which therapeutics to test. Realistically, this probably isn’t a single syndrome, and there are likely to be multiple underlying and mixed pathophysiologies and psychopathologies. This research needs to continue, but for now, paxlovid appears to be a drug fighting to find a reason for existence (and justification for the billions that have been spent on it).
Bottom line: Clearly, paxlovid should not be used for long COVID. Really, it isn’t clear that it should be used for anything at this point.
Cheesy joke of the month
I had a dream I was swimming in an ocean of orange soda. When I awoke I realized it was just a Fanta sea.
(I think a reader sent this one in at some point. Thanks! I always appreciate jokes in my in box.)