


Case
The 16 year old female with severe asthma you resuscitated last week ended up getting intubated. After calling the pediatric ICU you headed back into an overcrowded sea of belly pains and sprained ankles. 30 minutes later you are called overhead because the patient is now severely hypotensive and hypoxic…
My approach
The very first thing you do is disconnect the ventilator. If the problem was breath stacking, you will probably hear a loud and continuous hiss as the excess air escapes from the lungs.
Next, use a bag valve mask with end tidal CO2 attached. Using a BVM eliminates equipment problems and capnography should verify that the tube is not displaced. Remind yourself to bag slowly (so you aren’t causing breath stacking). Ensure that your BVM is hooked up to 100% oxygen. Bagging should also give you a sense of lung compliance.
Start a fluid bolus.
Next, assess the tube for obstruction. The best way to do this in a sick patient is to attempt to pass a suction catheter. If it passes easily, you have effectively ruled out obstruction as the problem. If it does not pass easily, you need to exchange the tube. If the patient is more stable, you can also check for obstruction with a fiberoptic scope.
Next, consider the possibility of pneumothorax. While bagging you can palpate the trachea and you can listen to the lungs, but these patients are moving so little air that diagnosing pneumothorax clinically may be challenging. In my mind, there are two options. For most patients, ultrasound is the ideal tool to rule out pneumothorax. (If you don’t know how, now is the time to learn. Check out the links at the bottom of this post for some excellent videos on ultrasound for pneumothorax.) If your patient is too sick to wait for an ultrasound, or if your machine is broken like mine always seems to be, the best move is to perform bilateral finger thoracostamies.
How do you perform a finger thoracostomy? It is really easy:
- Clean the skin
- Make a small (2cm) incision through the skin in the same position you would place a chest tube
- Bluntly dissect through the musculature with a kelly or with your finger
- Advance your finger through the parietal pleura
- If there was a gush of air, you can put a chest tube in later. If not, you ruled out pneumothorax and you can close and dress the skin when the patient is stable
At this point you have successfully run through the famous DOPES mnemonic:
- Displacement of tube
- Obstruction of tube
- Pneumothorax
- Equipment failure
- Stacked Breaths
If you have not discovered the reason for this patient’s hemodynamic collapse, you need to broaden your differential. I would start with my approach to the patient with undifferentiated hypotension and use the RUSH exam.
Of course, the best way to address peri-intubation hemodynamic collapse in an asthmatic patient is to prevent it from occurring in the first place:
Prevention
Even though we went over it last time, it is so important I am going to review it again here. In patients with status asthmaticus, a significant proportion of morbidity and mortality is directly related to mechanical ventilation. It is essential that you set the ventilator correctly to prevent these complications. The key is to prevent breath stacking by allowing a prolonged expiratory time. The three ways to increase the amount of exhaled air are:
- Increase the inspiratory flow rate. This allows the breath to be given over a shorter period of time and therefore allows more time to exhale
- Decrease the respiratory rate. The fewer breaths in per minute the more time you spend exhaling. The goal is to have an I:E (inspiratory to expiratory time ratio) of 1:4-5. In general, you are going to have to permit a degree of hypercapnia in order to maintain safe lung pressures. Hypercapnia is a significant stimulant, so remember to have an excellent sedation package
- Decrease the tidal volume. This has more to do with prevention of barotrauma, but again – the less air that is moving in, the easier it is to breath it out
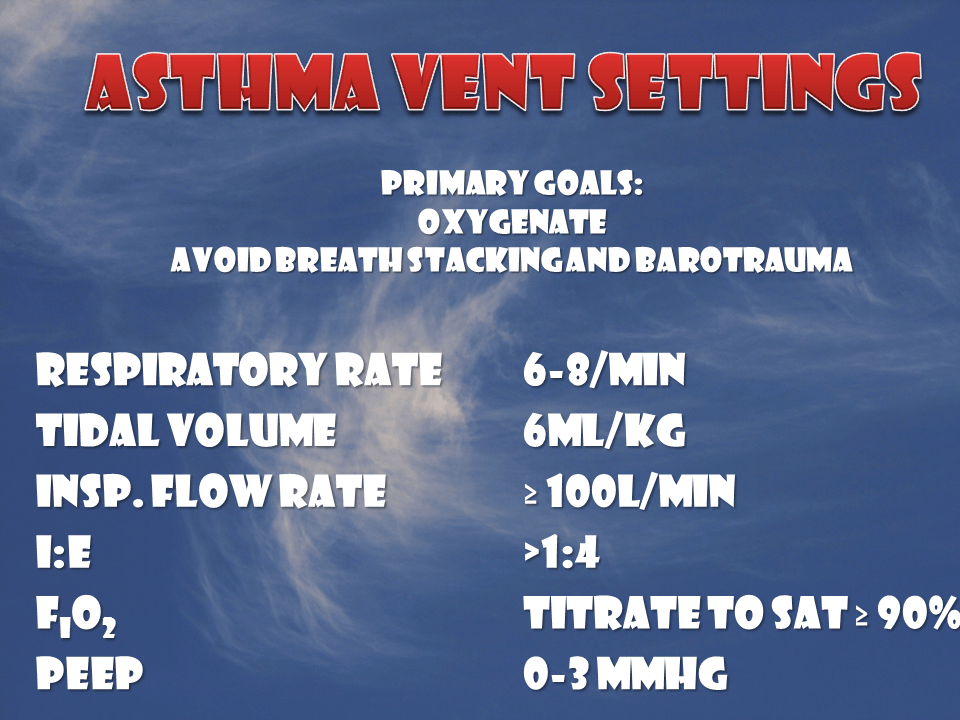
My initial vent settings:
- Respiratory rate of 6-8/min
- Tidal volume 6-8ml/kg ideal body weight
- Inspiratory flow rate ≥ 100L/min
- FiO2 100% (but rapidly titrating down to keep sats > 90%)
- PEEP: lowest my machine can set, or 0
Notes
Another mnemonic sometime used is DOTTS. It covers the steps to take when your intubated patient crashes:
- Disconnect – Disconnect patient from the ventilator
- Oxygen – Oxygenate patient with a BVM and feel for resistance as you bag
- Tube position/function – Did the ET tube migrate? Is it kinked or is there a mucus plug?
- Tweak the vent – Are the settings correct for this patient?
- Sonogram (ultrasound) – Sonogram to look for pneumothorax, mainstem intubation, etc.
Other FOAMed Resources
EMCrit Podcast 16 – Coding Asthmatic, DOPES and Finger Thoracostomy
EMCrit Lecture – Dominating the Vent: Part II
Mechanical Ventilation for Severe Asthma on Pediatric EM Morsels
Asthma and the Vent on the PEM ED podcast
The Crashing Asthmatic on Emergency Medicine Ireland
Some links for ultrasound for pneumothorax:
Lung and LV function from CastleFest 2013
Ultrasound for Detection of Pneumothorax on REBEL EM
Pneumothorax on Mount Sinai Emergency Medicine Ultrasound
References
Papiris S, Kotanidou A, Malagari K, Roussos C. Clinical review: severe asthma. Crit Care. 2002;6:(1)30-44. PMID: 11940264 [Free Full Text]
Stanley D, Tunnicliffe. Management of life-threatening asthma in adults. Contin Educ Anaesth Crit Care Pain (2008) 8 (3): 95-99. [Free Full Text]
Deakin CD, Davies G, Wilson A. Simple thoracostomy avoids chest drain insertion in prehospital trauma. J Trauma. 1995;39:(2)373-4. PMID: 7674410
Morgenstern, J. Post-intubation deterioration in asthma, First10EM, August 24, 2015. Available at:
https://doi.org/10.51684/FIRS.672