
COVID-19 has resulted in many conflicting messages. One area of extreme importance is the health and safety of healthcare workers. I have repeatedly heard that our infection control measures are perfect, and cannot be questioned, while simultaneously seeing numerous colleagues contract the virus. When it comes to the safety of our healthcare workers, opinion is not good enough, and the science is pretty clear: we are not doing enough to protect healthcare workers from COVID-19.
The evidence
Healthcare workers are disproportionately contracting COVID-19. Based on a review done in April, the rate of documented COVID-19 infection was 9-10 times higher among healthcare workers than in the general population. (Otto 2020) This was true regardless of the country being studied, although the rate was higher in regions with higher rates of COVID-19 or strained healthcare systems.
A preprint publication of a prospective cohort from 2 university hospitals in New Jersey found a 7% absolute increase in the risk of COVID-19 among healthcare workers (or a 1825% relative risk increase) as compared to non-healthcare workers also working in the hospital but without direct patient care responsibilities. Test positivity was higher in healthcare workers, so the results can’t be blamed on ascertainment bias. (Discussed further below). The majority of healthcare workers infected were nurses (63%), which makes sense as they are the group that spends the longest time with patients and therefore have the highest cumulative viral exposure. The rate of infection was 11% in nurses, 2% in attending physicians, and 3% in resident physicians. Only half of the healthcare workers reported wearing PPE for all patient encounters, but the rate of infection was actually a little higher in the group of individuals with 100% PPE use (9.3%). ICU workers had lower rates of infection than those working in other units (2% vs 5-10%), which is a recurrent and potentially important observation. Emergency department staff had the same risk as everyone else (8.3%). (Barrett 2020)
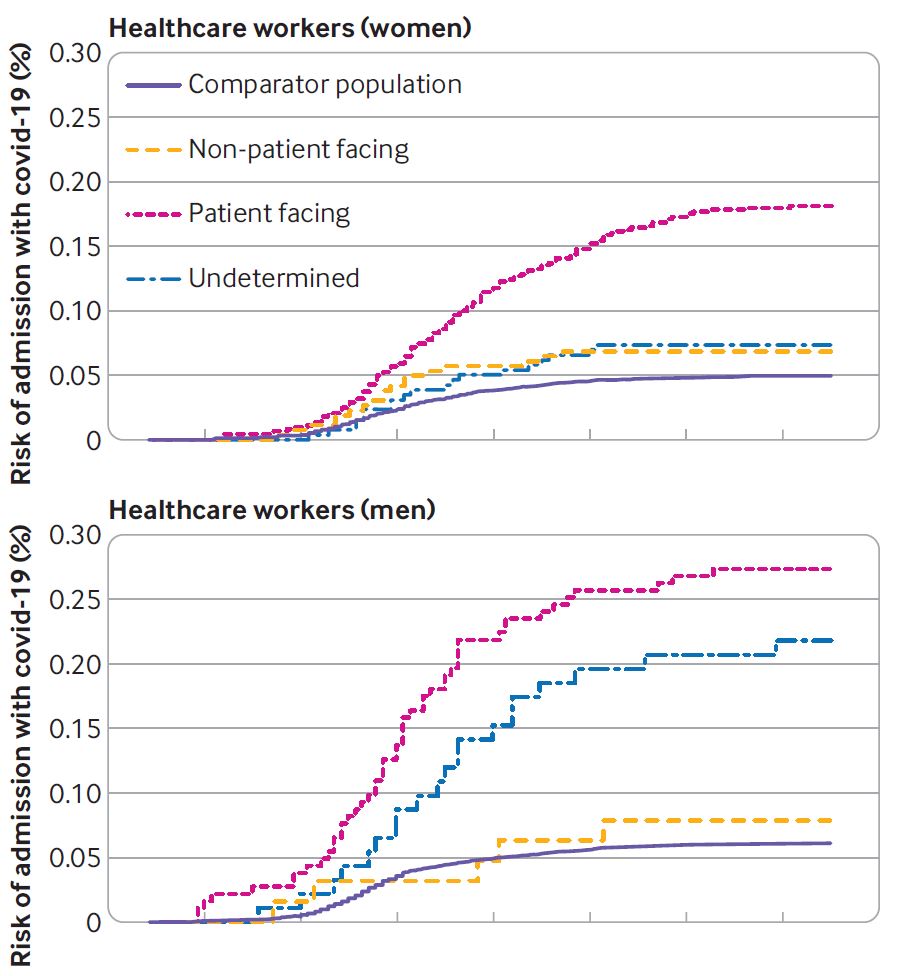
In a large database study looking at the entire population of Scotland between March 1 and June 6, 2020, 17.2% of hospital admissions among working age individuals occurred among healthcare workers or their family members, despite this group accounting for only 11.2% of the total population. (Shah 2020) Healthcare workers in “non-patient facing roles” had a risk similar to the general population. Healthcare workers in “patient facing roles” were significantly more likely to be admitted to hospital with COVID-19 (hazard ratio 2.09, 95% CI 1.49-2.94). The absolute risk of being admitted to hospital with COVID-19 was 0.5%. In total, there were 6346 patients admitted to hospital in this period in Scotland, and with a population of 5,463,300, this translates to an absolute risk of 0.1% (including the healthcare workers). I think the numbers will be an under-estimate of the actual risk, because healthcare workers are likely to be healthier than the general population, and therefore less likely to require admission if they are infected with COVID-19. The absolute numbers are small, but one in eight of these healthcare workers required admission to critical care and 6 of our colleagues died.
There are numerous other studies, all with the same conclusion: healthcare workers are much more likely than the general population to contract COVID-19. (Nguyen 2020, Pouwels 2020, Pollán 2020, Iversen 2020; Quigley 2020)
Allow me to pause and emphasize something that is incredibly important, but is easy to lose track of as I present a slew of numbers. These are people. These are our colleagues. These are not statistics. There are healthcare workers losing their lives while trying to save the lives of others.
The absolute numbers are rather staggering. As of July 16th, there had been 2,633,585 COVID cases in the United States. Occupation data was only available for 571,708 patients (22%), and of this group there were more than 100,000 healthcare workers who had contracted COVID, and 641 healthcare workers who had died of COVID-19. If the numbers are extrapolated to the entire cohort, that would translate to more than 450,000 healthcare workers who had contracted COVID-19 and almost 3,000 who had died by mid-July in the United States alone! (Although it is likely that there are fewer healthcare workers among the patients for whom an occupation was unknown, so a direct extrapolation is probably inaccurate.) (Hughes 2020)
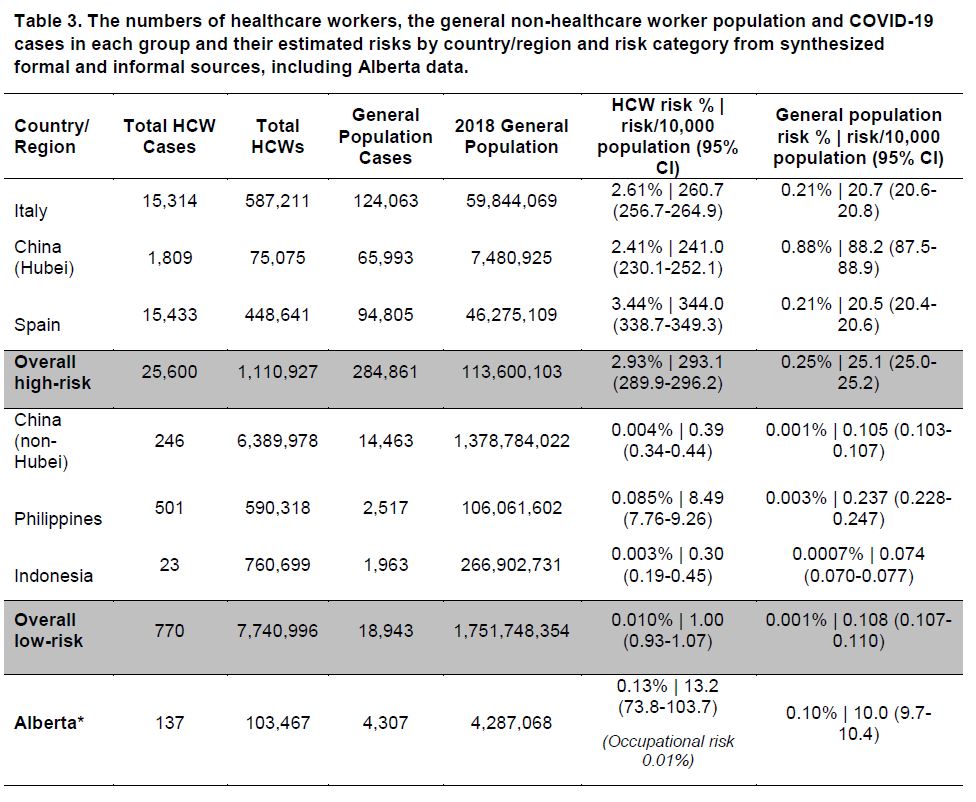
The absolute risk to healthcare workers will depend on the overall prevalence of COVID-19 in the community. Overall, the absolute risk is low, but 2.5-3.5% of healthcare workers were infected during the first wave in Spain, Italy, and Hubei. Whatever the setting, the risk in healthcare workers is much higher than the risk in the general population. If the absolute risk is low, it is simply because there is not a lot of COVID-19 going around. (Otto 2020) That does not bode well for the massive second waves we are currently seeing around the world.
I could not find any direct comparisons of different infection control practices, but different countries have developed very different approaches to this disease, and it appears that some may be better than others. For example, one hospital in Singapore, which has managed 748 COVID-19 cases, employed PAPRs (powered air-purifying respirators) for all healthcare workers working in the emergency department, ICU, operating theatre, isolation wards, and endoscopy centre. They report 0 healthcare worker infections with COVID-19. (Koh 2020) Similarly, at 4 hospitals in Wuhan where N95 masks and surgical masks were both worn at all times, in addition to other measures, they did serologic testing of 420 frontline healthcare professionals (80% of whom worked in critical care), and none were positive. (Liu 2020) There are many other informal reports that Asian countries in particular are using much more stringent PPE than we are in North America, and seem to have lower healthcare worker infection rates, but unfortunately formal data in this realm is severely lacking.
Discussion
The exact risk is unknown
I think these numbers may be an underestimate the real risk to healthcare workers. The workload in hospitals dropped dramatically during the first wave. Elective surgeries were cancelled. Patients were asked to stay home. Lockdowns prevented many of the activities that usually bring people to the emergency department. Many physicians had closed their offices. The reported infection rates come from a time when many physicians weren’t in the hospital; weren’t seeing patients in person. They come from a time when emergency departments were much more empty and patients didn’t have to be seen in hallways. They come from a time when there were fewer patients around in general, which translates to fewer aerosols, and less opportunity for infection.
The risk is likely to be higher during the second wave. We are seeing a tremendous increase in workload. Hospitals don’t want to shut down again – in fact, we are working hard to catch up on the many missed surgeries and visits. Hospitals are back above capacity, and emergency hallways are filling up. We always work hard, but are working harder than ever. We are exhausted and more likely to make mistakes. All of this matters a lot when interpreting infection rates, and is why I think we should expect an even higher rate of healthcare infection during the second wave.
However, the opposite argument could also be made. Some of this data comes from health systems that were overwhelmed. Some of it comes from a time when PPE was in very short supply, and people may not have been properly fit for N95 masks and trained on all infection control practices. Therefore, you might optimistically hope that the infection rate will be lower with time, but that assumes that our current infection control practices are working, and the massive increased risk faced by healthcare workers suggests that they aren’t.
Who is defined as a healthcare worker?
A major problem in all of these studies is determining exactly who is defined as a healthcare worker. Some people will be overlooked. For example, the ortho-techs in our emergency department have face to face interactions with a large number of emergency department patients every day, but (ridiculously) aren’t defined as “frontline workers”, and therefore don’t get the COVID pay that others are healthcare workers are getting. On the other hand, many healthcare workers will not actually be at higher risk for contracting COVID-19. Many physicians have closed their offices and are providing virtual care. Many physicians work with very low risk populations. These individuals are all included in the denominator of these studies. The risk for high risk healthcare workers – such as those working in the emergency department – will likely be significantly higher than the average numbers reported here.
Are people actually catching COVID in the hospital?
When faced with healthcare worker infections, it is common for hospitals to deny responsibility, claiming that the infection must have been contracted outside of the hospital. Although some individuals will get sick outside the hospital, the numbers suggest that most people are in fact getting sick at work.
We can’t know for sure where any individual contracted the virus. One report suggests that 55% of healthcare workers who had confirmed contact with a COVID-19 case were exposed through work. (CDC COVID-19 Response Team 2020) However, on the whole, I think claims like this are likely to be inaccurate and biased. It is almost impossible to determine where one was infected (although genetic studies looking at strains could potentially help). Individuals investigating these cases often have biased perspectives, such as needing to prove their hospital’s infection control policies are safe. Participants in the studies will have significant recall bias. The numbers could be wrong in either direction. I don’t think these estimates can be relied on.
If healthcare workers were getting sick in the community, the incidence of infection in healthcare workers should be close to the incidence in the community. It is not even close. The studies above suggest that healthcare workers are 2 to 10 times more likely to contract COVID-19 than individuals in the general population. With numbers that high, it is outrageous to claim that healthcare workers are not contracting this disease through workplace exposures. Considering these numbers, if a healthcare worker becomes sick, workplace exposure should be the assumption, and community spread must only be a diagnosis of exclusion.
Ascertainment bias?
Healthcare workers may have greater access to testing than the general population, which could bias the numbers, but I don’t think the available data suggests that the massive increase in healthcare worker infections is due to increased testing. For example, in the study done in New Jersey, the rate of test positivity was much higher in healthcare workers than non-healthcare workers. (Barrett 2020) If healthcare workers were being over-tested, we would expect to see more negative test results, and therefore a lower test positivity rate. It is true that healthcare workers are getting tested more often, but that might simply be because they are getting sick more often.

The data from Scotland also argues against a major role of ascertainment bias, because that study focus only on hospitalizations. (Shah 2020) Extra testing may increase the identification of individuals with milder symptoms, but will have no effect on the hospitalization rate.
What is the role of compliance?
Without a doubt, poor adherence to infection control guidelines will explain some of these infections. Doffing and donning properly isn’t easy. Like everyone else in 2020, healthcare workers are fatigued, and simple lapses are not uncommon. However, I think it is wrong to blame healthcare worker infections on compliance.
It is just too easy an excuse. It prevents us from looking into the root causes. It is a way for the individuals in charge of infection control practices to absolve themselves of responsibility. They end up blaming the victim rather than looking for holes in the protocols. One thing should be clear: if people are getting sick, there are massive holes in our protocols. One possibility is that our current protocols are inadequate, which might be the case if, for example, they are not adequately accounting for the role of aerosol spread of COVID-19. (And this seems to be suggested by the lack of healthcare worker infections in the hospitals using PAPRs and N95s mentioned above.) Another possibility is that the protocols are theoretically perfect, but fail in implementation. Either way, it is not the user’s fault. For something as important as keeping healthcare workers healthy, the protocols must be designed so that they cannot possibly fail. Sadly, it is clear from this data that they are not.
Of course, the responsibility doesn’t lie solely with infection control teams. I worry that individuals have been too heavily blamed for getting sick during this pandemic, but it’s true that we all have a responsibility. We have a responsibility to ourselves and to our colleagues. If we see someone making a mistake in infection control practices, it is our responsibility to point it out. It is our responsibility to set a good example. It is our responsibility to think about our work spaces, and make sure that they are safe for staff and patients alike. We cannot blame individuals for catching COVID, but we must do absolutely everything in our power to ensure they don’t.
What can we do?
Healthcare workers have been disproportionately impacted by COVID-19 and we need to remedy that problem immediately. Unfortunately, the exact remedy is unclear.
The first order to business is to fill in the significant gaps in our knowledge about SARS-CoV-2 transmission. There is still so much we don’t know. We still don’t know exactly what role aerosols play in the spread of the disease. We aren’t sure what procedures count as aerosol generating. We still don’t know which activities place healthcare workers at the highest risk. There are no large scale studies comparing different PPE strategies. We can’t solve the problem of disproportionate healthcare worker infections without better science explaining why we are getting sick. We have dumped mountains of research dollars into unlikely therapies like hydroxychloroquine, but embarrassingly little into the basic question of how to keep our frontline workers safe. That needs to change quickly. High quality studies evaluating our infection control practices are absolutely essential to protect healthcare workers and their families. (Karlsson 2020)
What do we do in the meantime? First, we need to acknowledge that this is a problem. Healthcare workers are getting sick at work. We can’t deny that fact.
We need humility. Black and white statements like “you are safe if you are more than 2 meters away from the patient” or “procedure X is definitely not aerosol generating” are almost always scientifically unfounded. (This is especially galling when there is evidence from SARS that many of the procedures being declared “not aerosol generating” – such as CPR and the use of a nonrebreather – were associated with increased risk of infection among healthcare workers.) (Liu 2009; Loeb 2004)
It is unreasonable and dangerous to pretend that we know exactly how to prevent this disease while simultaneously watching so many of our colleagues getting sick at work. These black and white statements have led to ridiculous policies in many hospitals. The insistence that the disease is purely droplet spread, and that you are safe as long as you are 2 meters away from the patient, results in the door being left open to the room containing the the febrile coughing patient on a nonrebreather, because his bed is 3 meters away from the nursing station and therefore “safe”. It costs nothing to close a door. It may (in fact, it probably does) add a significant level of protection, but it is taboo in the hospital because it implies that you don’t believe in the 2 meter rule that infection control and administration have repeatedly sworn is 100% effective.
We need to be stringent in our application of current infection control guidelines, but also remain open to the possibility that they need to change. We need to vigorously investigate every healthcare worker illness, looking for gaps in our current system. When there is low hanging fruit (such as closing doors when patients have respiratory illnesses), we need to embrace those efforts, even if they aren’t part of current protocols, and even if the evidence is imperfect.
We need to take responsibility for our own safety, and also the safety of the people around us. We need to set a good example. We need to wear our PPE and not cut corners. However, we absolutely must not blame healthcare workers if they become ill. That is a system failure, not a personal one.
When a vaccine is available, we must ensure vaccinating healthcare workers is a priority.
A minor stop-gap that is suggested in these papers is to move high risk healthcare workers to non-patient facing jobs, as the rate of COVID-19 in non-patient facing healthcare workers appears to be about the same as the general population. (Shah 2020) However, I think it is our job to protect all healthcare workers, whatever their baseline risk.
Perhaps the single greatest thing we can do to protect healthcare workers is to adopt a “zero COVID” strategy in our countries; to institute much more stringent measures now, with the lofty goal of eliminating community spread of the disease. Simply allowing COVID to spread in the community is a clear statement that, despite all the parades and well wishes, our society truly does not value the lives of its frontline healthcare workers.
Personally, I don’t think any healthcare worker should be expected to contract COVID-19 in the course of their job. Our health and safety must come first. However, these numbers suggest we are failing in that goal.
Conclusion
Healthcare worker safety should be a top priority of our pandemic response. Healthcare workers should not have to face illness and potential death when caring for patients. As if that wasn’t enough, sick healthcare workers cannot work, adding another stress to an already overburdened healthcare system. The science is clear: healthcare workers are disproportionately afflicted by COVID-19. Unfortunately, we don’t fully know why.. We urgently need better data addressing the source of this risk and its mitigation. However, we cannot simply sit by and wait for data. Our colleagues are dying, and the time for action is now.
Other FOAMed
St Emlyn’s: Why infection control failures might kill your patients and colleagues
Other COVID-19 resources on First10EM
References
Barrett ES, Horton DB, Roy J, et al. Prevalence of SARS-CoV-2 infection in previously undiagnosed health care workers at the onset of the U.S. COVID-19 epidemic [Internet]. Infectious Diseases (except HIV/AIDS); 2020 [cited 2020 Nov 14]. Available from: http://medrxiv.org/lookup/doi/10.1101/2020.04.20.20072470
CDC COVID-19 Response Team. Characteristics of Health Care Personnel with COVID-19 – United States, February 12-April 9, 2020. Morbidity and Mortality Weekly Report (MMWR), 2020;69(15), 477–481. Retrieved from https://www.cdc.gov/mmwr/volumes/69/wr/mm6915e6.htm?s_cid=mm6915e6_w
Hughes MM, Groenewold MR, Lessem SE, et al. Update: Characteristics of Health Care Personnel with COVID-19 — United States, February 12–July 16, 2020. MMWR Morb Mortal Wkly Rep 2020;69:1364–1368. DOI: http://dx.doi.org/10.15585/mmwr.mm6938a3external icon
Hunter E, Price DA, Murphy E, van der Loeff IS, Baker KF, Lendrem D, Lendrem C, Schmid ML, Pareja-Cebrian L, Welch A, Payne BAI, Duncan CJA. First experience of COVID-19 screening of health-care workers in England. Lancet. 2020 May 2;395(10234):e77-e78. doi: 10.1016/S0140-6736(20)30970-3. Epub 2020 Apr 22. PMID: 32333843
Iversen K, Bundgaard H, Hasselbalch RB, Kristensen JH, Nielsen PB, Pries-Heje M, Knudsen AD, Christensen CE, Fogh K, Norsk JB, Andersen O, Fischer TK, Jensen CAJ, Larsen M, Torp-Pedersen C, Rungby J, Ditlev SB, Hageman I, Møgelvang R, Hother CE, Gybel-Brask M, Sørensen E, Harritshøj L, Folke F, Sten C, Benfield T, Nielsen SD, Ullum H. Risk of COVID-19 in health-care workers in Denmark: an observational cohort study. Lancet Infect Dis. 2020 Aug 3:S1473-3099(20)30589-2. doi: 10.1016/S1473-3099(20)30589-2. Epub ahead of print. Erratum in: Lancet Infect Dis. 2020 Oct;20(10):e250. PMID: 32758438
Karlsson U, Fraenkel C. Covid-19: risks to healthcare workers and their families BMJ. 2020;
Koh FH, Tan MG, Chew MH. The fight against COVID-19: disinfection protocol and turning over of CleanSpace® HALO™ in a Singapore Hospital. Updates Surg. 2020 Jun;72(2):311-313. doi: 10.1007/s13304-020-00809-3. Epub 2020 May 27. PMID: 32462609
Liu M, Cheng SZ, Xu KW, Yang Y, Zhu QT, Zhang H, Yang DY, Cheng SY, Xiao H, Wang JW, Yao HR, Cong YT, Zhou YQ, Peng S, Kuang M, Hou FF, Cheng KK, Xiao HP. Use of personal protective equipment against coronavirus disease 2019 by healthcare professionals in Wuhan, China: cross sectional study. BMJ. 2020 Jun 10;369:m2195. doi: 10.1136/bmj.m2195. PMID: 32522737
Liu W, Tang F, Fang L, et al. Risk factors for SARS infection among hospital healthcare workers in Beijing: a case control study . 2009; 14:52-59.
Loeb M, McGeer A, Henry B, et al. SARS among critical care nurses, Toronto. Emerg Infect Dis. 2004;10(2):251–255. doi:10.3201/eid1002.030838 PMID: 15030692
Nguyen LH, Drew DA, Joshi AD, et al. Risk of COVID-19 among frontline healthcare workers and the general community: a prospective cohort study. medRxiv [Preprint]. 2020 May 25:2020.04.29.20084111. doi: 10.1101/2020.04.29.20084111. Update in: Lancet Public Health. 2020 Jul 30;: PMID: 32511531
Otto S, Babujee A, Neustaedter C, et al. COVID-19 Risk to Healthcare Workers. Alberta Health Services, COVID-19 Scientific Advisory Group. April 8, 2020. (Version 1)
Otto S, Babujee A, Neustaedter C, et al. COVID-19 Risk to Healthcare Workers. Alberta Health Services, COVID-19 Scientific Advisory Group. May 4, 2020. (Version 2) Available here: https://www.albertahealthservices.ca/assets/info/ppih/if-ppih-covid-19-hcw-risk-rapid-review.pdf
Pollán M, Pérez-Gómez B, Pastor-Barriuso R, et al. Prevalence of SARS-CoV-2 in Spain (ENE-COVID): a nationwide, population-based seroepidemiological study The Lancet. 2020; 396(10250):535-544.
Pouwels KB, House T, Robotham JV, et al. Community prevalence of SARS-CoV-2 in England: Results from the ONS Coronavirus Infection Survey Pilot. 2020. https://www.medrxiv.org/content/10.1101/2020.07.06.20147348v1
Quigley AL, Stone H, Nguyen PY, Chughtai AA, MacIntyre CR. Estimating the Burden of COVID-19 on the Australian Healthcare Workers and Health System International Journal of Nursing Studies. 2020; https://doi.org/10.1016/j.ijnurstu.2020.103811
Ran L, Chen X, Wang Y, Wu W, Zhang L, Tan X. Risk Factors of Healthcare Workers With Coronavirus Disease 2019: A Retrospective Cohort Study in a Designated Hospital of Wuhan in China . 2020;
Shah ASV, Wood R, Gribben C, Caldwell D, Bishop J, Weir A, Kennedy S, Reid M, Smith-Palmer A, Goldberg D, McMenamin J, Fischbacher C, Robertson C, Hutchinson S, McKeigue P, Colhoun H, McAllister DA. Risk of hospital admission with coronavirus disease 2019 in healthcare workers and their households: nationwide linkage cohort study. BMJ. 2020 Oct 28;371:m3582. doi: 10.1136/bmj.m3582. PMID: 33115726
Morgenstern, J. We are not doing enough to protect healthcare workers from COVID-19, First10EM, November 23, 2020. Available at:
https://doi.org/10.51684/FIRS.51897




4 thoughts on “We are not doing enough to protect healthcare workers from COVID-19”
Amen and thank you!! We need THIS kind of discourse that is passionate about the facts and keeping people safe, dispassionate about politics!
Thank you First10EM!!!!!
Dr. Morgenstern,
Hopefully, you are already aware of this, but if not…Great news! There is now tested a mask to stop 100% of all staff infections inside of hospital COVID-19 wards! Please see the news from a clinical study in Cambridge, England. https://www.theguardian.com/world/2021/jun/29/cambridge-hospitals-mask-upgrade-appears-to-eliminate-covid-19-risk-to-staff?CMP=fb_gu&utm_medium=Social&utm_source=Facebook#Echobox=1624956011
Best Regards,
Claudio H. Caycedo DDS/ Aerospace Engineer