The COVID-19 pandemic has resulted in a tidal wave of new information, research, and guidance. On one hand, I think this is a remarkable example of our ability as a medical community to respond to a crisis and the value of social media channels for the rapid dissemination of information. On the other hand, it is almost impossible to keep up, and different recommendations seem to conflict, increasing anxiety of front line providers. I have written before about some of the many reasons that I hate guidelines. In particular, guidelines that obscure the reasoning or science behind their recommendations, or which make strong recommendations based on weak science, can create confusion and paradoxically hurt patient care. With the rapid emergence of COVID, there is very little strong science, and so it is particularly important to be careful about our guidelines and their potential unintended consequences. We need to openly discuss the science (or lacking science, logic) behind the recommendations. When recommendations are weak, that needs to be clear, because we may need to rapidly alter clinical plans as the pandemic progresses. With all that said, I will provide a quick summary of my main take-aways from the Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). Like all the papers I discuss on this blog, I strongly suggest that you read the paper for yourself (assuming you can find the time away from managing all the sick patients.)
The paper
Alhazzani W, Moller MH, Arabi YM, et al. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19). 2020. Preprint, available here, downloaded March 22, 2020.
My Summary
PPE
The PPE statements are pretty straightforward, and hopefully uncontroversial. (However, they are incredibly important, so I will quote them in their entirety):
- “For healthcare workers performing aerosol-generating procedures on patients with COVID-19 in the ICU [I will add: OR ANYWHERE ELSE], we recommend using fitted respirator masks (N95 respirators, FFP2, or equivalent), as opposed to surgical/medical masks, in addition to other personal protective equipment (i.e., gloves, gown, and eye protection, such as a face shield or safety goggles) (best practice statement).
- We recommend performing aerosol-generating procedures on ICU patients with COVID-19 in a negative pressure room (best practice statement).
- For healthcare workers providing usual care for non-ventilated COVID-19 patients, we suggest using surgical/medical masks, as opposed to respirator masks, in addition to other personal protective equipment (i.e., gloves, gown, and eye protection, such as a face shield or safety goggles) (weak recommendation, low quality evidence).
- For healthcare workers who are performing non-aerosol-generating procedures on mechanically ventilated (closed circuit) patients with COVID-19, we suggest using surgical/medical masks, as opposed to respirator masks, in addition to other personal protective equipment (i.e., gloves, gown, and eye protection, such as a face shield or safety goggles) (weak recommendation, low quality evidence).”
Intubation
They recommend video laryngoscopy over direct, if available, but it is a weak recommendation based on the idea that it might increase first pass success. They also suggest that the intubation be performed by the healthcare worker with the most experience in airway management.
Fluid therapy
Perhaps their most important recommendation, and the one that may represent a big practice change for some people is: “For the acute resuscitation of adults with COVID-19 and shock, we suggest using a conservative over a liberal fluid strategy (weak recommendation, very low quality evidence).” The amount of intravenous fluid we have been using in resuscitation has been trending down for a while, but if you are someone who still reflexively orders 30 mL/kg for every sepsis patient, this might be the time to reassess that practice. (Excess fluids are particularly bad for ARDS patients.)
They also make the unsurprising recommendation to use crystalloids over other options. They like balanced crystalloids, but I still don’t think there is any good evidence that normal saline results in worse outcomes.
Vasopressors
Norepinephrine is the first line agent for septic shock. If norepinephrine is not available, epinephrine or vasopressin would be their replacement first line agents. (Both weak recommendations.)
They make a strong recommendation against using dopamine. Again, I think most of us have moved away from dopamine over the years, as there is good evidence of increased adverse events, and weak evidence that it might increase mortality.
As a goal, they recommend a MAP between 60 and 65, rather than anything higher. They recommend vasopressin as the second line agent, rather than high doses of norepinephrine. Hopefully this is more of an ICU decision than an ED decision, but if there is evidence of cardiac dysfunction, they suggest adding dobutamine.
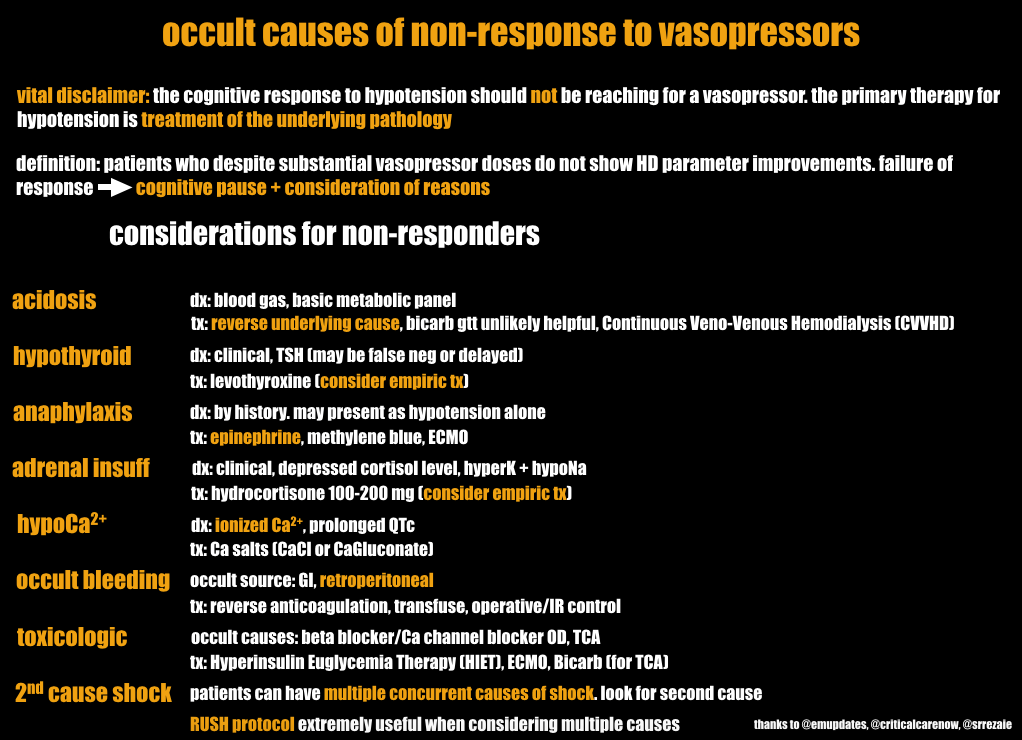
For refractory shock, they suggest adding low dose corticosteroid therapy. (For refractory shock, I would also suggest broadening your differential to make sure something other than sepsis wasn’t missed. I particularly like Salim Rezaie’s checklist for occult causes of non-response to vasopressors:
Ventilatory support
For some reason, they have 2 different cutoffs for starting oxygen therapy (92% and 90%). One gets a “suggest” and one gets a “recommend”. I would never start oxygen just to treat a sat of 91%, so let’s stick with their recommendation of less than 90% (although I wonder if we can’t even go a little lower than that in some clinical circumstances). They call this a strong recommendation with moderation evidence, but the only evidence cited is that liberal oxygen is associated with bad outcomes.
They make a strong recommendation to target an oxygen saturation no higher than 96%.
Then, things start getting a little more controversial, and you will notice deviation from some of the guidelines we are currently using in Canada.
- They suggest highflow nasal cannula (HFNC) over both conventional oxygen therapy and noninvasive positive pressure ventilation in patients who are hypoxic despite conventional oxygen therapy. (We are currently suggesting against these devices. Their recommendation is weak, based on a low quality of evidence, and therefore so is ours.) They present some evidence that HFNC reduces intubation, that there was no increased risk of transmission from HFNC during SARS, and that in studies of bacterial pneumonia, the combination of the room is the same with HFNC as it is with conventional oxygen.
- They are also making a weak recommendation to use non-invasive positive pressure ventilation if the patient doesn’t have an urgent indication for intubation, and HNFC is not available. This requires close monitoring for deterioration and a readiness to intubate if needed. They acknowledge that experience with MERS was that NIPPV has a high failure rate (92%) and that it is a aerosol generating procedure that was associated with the spread of SARS. They say the balance between the risks and benefits are unclear.
These are probably the two most controversial recommendations. Our current advice is to avoid them both to limit risk to healthcare providers. However, we are hearing from experts in places that have already been hit hard by this (China, Italy, and New York City) that the early intubation strategy is likely to fail because you will quickly have more patients than ventilators. Using these non-invasive strategies can free up ventilators, and they can probably be used safely if you have negative pressure rooms and appropriate PPE. The evidence is weak either way, but I think it is important to know that this is one of the recommendations that might have to change with time, depending on how the pandemic progresses.
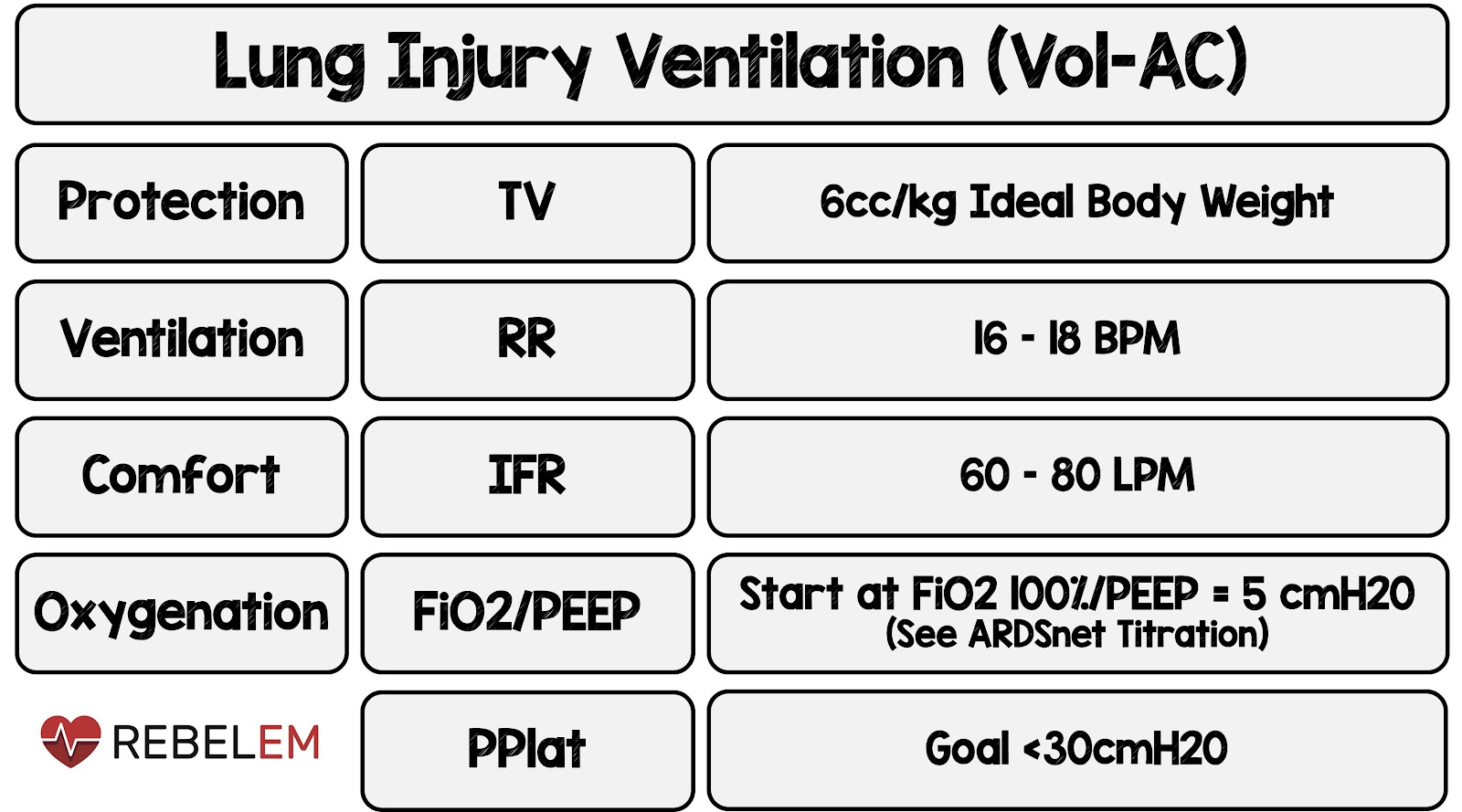
In terms of ventilation, we should be using the classic ARDS lung protective strategies that hopefully everyone knows by now. That means using low tidal volumes (4-8 mL/kg IDEAL body weight), targeting plateau pressures less than 30 cm H2O, and following a higher PEEP strategy, like the one outlined in the classic ARDSnet trial:

I like the graphics from Salim Rezaie:

They make some other ICU recommendations, like the use of proning. In terms of emergency department management, the last really important recommendation is that in mechanically ventilated patients, they suggest empiric antibiotics. In our sickest patients that seems reasonable, although for most patients, this is viral so antibiotics aren’t going to do anything. They also make the recommendation to treat fever, despite reasonably good evidence that treatment fever in the ICU doesn’t help. They recommend specifically against using convalescent serum, and for all the other experimental treatments you might be hearing about (antivirals and hydroxychloroquine), they say there is not enough evidence to make a recommendation, and my take is these clearly shouldn’t be used outside of an clinical trial.
Other FOAMed
FOAMCast: COVID-19: Society of Critical Care Medicine Surviving Sepsis Guidelines #COVID19
You can find more information about COVID 19 here.
Morgenstern, J. Surviving Sepsis Campaign COVID Guidelines, First10EM, March 27, 2020. Available at:
https://doi.org/10.51684/FIRS.16370



One thought on “Surviving Sepsis Campaign COVID Guidelines”
I do not understand most recommendations about O2. O2 sats in the low 90s are normal here in Colorado. Sats in the high 70s are normal at 18,000 feet. These sats decrease exercise tolerance but seem to cause no real problems after a short acclimatization period. Unless higher O2 improves clinical outcomes (which there is little data about) or the patient is symptomatic I suspect sats in the 80s are fine.