
Morgenstern, J. Research Roundup (May 2022), First10EM, May 2, 2022. Available at:
https://doi.org/10.51684/FIRS.127236
Another month, another collection of (hopefully) interesting medical publications.
When trial results are too good to be true, think fraud?
Sheldrick, K. Evidence of Fabricated Data in a Vitamin C trial by Paul E Marik et al in CHEST. Available at: https://kylesheldrick.blogspot.com/2022/03/evidence-of-fabricated-data-in-vitamin.html
This is the first time I have ever included a blog post in these EBM summaries, but I think both the content and the concept are incredibly important. I have discussed the whole vitamin C in sepsis thing many times before. When it comes to the original Marik study, my quote was “the results of this trial are unbelievable. Seriously, the massive difference in mortality is literally not believable.“ This blog post is a copy of a letter that was sent to the editor of Chest alleging research fraud in the original Marik paper. That is obviously a very serious allegation, and I have no special insight into the veracity of the claim. However, statistical methods have been very successful at identifying datasets that are so implausible that they are essentially impossible. This is how the key ivermectin study was initially found to be fraudulent, among many other examples. This author looks at the statistics of “table 1” in the Marik study, and concludes “there is simply no explanation for this other than fraud.” Why would I include a blog post / letter to the editor like this? 1) I think it is important to remember that fraud is a relatively common occurrence in medical science, and we always need to adjust our confidence based on the possibility. 2) I think it is important to know that statistical tools exist to identify fraud. 3) I think it borders on being negligent that none of those tools are routinely employed by editors or peer reviewers at major journals. How exactly do they justify their massive journal fees? In the era of electronic publication, why do we even need journals anymore? They clearly do nothing to elevate the level of scientific discussion.
Bottom line: It sounds like the original Marik study might have been fraudulent, which combined with the many negative RCTs since, basically puts the final nail in the metabolic cocktail coffin. (If fraudulent, it also resulted in a massive amount of wasted research dollars. I have never heard of someone being held liable for such a scenario, but it is an interesting thought.)
UPDATE: I want to be clear that I don’t know enough about this statistical analysis to know whether it holds water. I have had multiple incredibly smart researchers reach out to say that they have problems with the analysis. There is a great discussion section on the original blog post that demonstrates that different assumptions can result in very different outcomes. (They all still seem to say that data is unlikely, but there is a big difference between a 1 in 1000 dataset, which will happen regularly given how much research is published, and an infinitely unlikely dataset.) I included it because I think fraud, and the statistical tools available to detect it, are important and interesting topics of conversation. It may have been more prudent to wait for a response from Chest and Dr. Marik before including it in a blog post, especially seeing as this practice has been well debunked with proper RCTs at this point, so this analysis is unlikely to change clinical practice. However, it is here now, so just interpret with caution.
Peripheral IVs post mastectomy: Another medical myth?
Naranjo J, Portner ER, Jakub JW, Cheville AL, Nuttall GA. Ipsilateral Intravenous Catheter Placement in Breast Cancer Surgery Patients. Anesth Analg. 2021 Sep 1;133(3):707-712. doi: 10.1213/ANE.0000000000005597. PMID: 34043309
The idea that a peripheral IV on the same side of the body as prior breast surgery could cause significant harm always struck me as rather ridiculous. The veins are still intact. Large volumes of blood still flow through those veins on a daily basis. Was a small amount of fluid from an IV really going to make a difference? This is a chart review that identified 3724 patients with prior surgery for breast cancer who underwent 7896 IV placements for surgery or anesthesia. These IVs were being placed a median of 1.5 years after the original breast cancer surgery. The complications they were looking for were venous thrombosis, cellulitis, and breast cancer related lymphedema. Complications were incredibly rare overall, with a rate of only 5 per 10,000. Interestingly, in this hospital more IVs were placed in the ipsilateral arm (5153) than the contralateral arm (2743), so obviously this hospital doesn’t believe the dogma. There were 2 complications in both groups, a rate of 7.2 per 10,000 in the contralateral arm and 3.9 per 10,000 in the ipsilateral arm, with no statistical significance. Interestingly, both complications in the contra-lateral group were lymphedema on the opposite side of the body. In other words, it is the salty water you are putting into the body that causes the edema (or the general inflammatory state caused by surgery), but not the position of the IV itself. All 4 women with complications had a prior history of lymphedema, so it makes sense to be cautious in these patients, no matter where you place the IV. That being said, the rate is still very very low. Of course, this is a chart review, so there are significant limitations. We can’t be sure that every IV and every complication was identified. More importantly, there may be significant confounders. We don’t know why clinicians decided to use one arm or the other. It is possible that RNs placed routine IVs, but ipsilateral IVs were considered complex, so they were done by anesthesiologists. (I am not sure why that would matter, but the point is the data set is messy.) However, despite those limitations, I think the overall conclusion is going to be correct. Even if ipsilateral IVs had double the rate of complications, when you are starting at a rate of 5 in 10,000, and all these complications self resolved, this is well within the range of an acceptable risk, or at least one that can be discussed with patients for shared decision making. Apparently this is not new information. (If you dig back far enough, it sounds like this practice stems from a handful of case reports in the 1950s after radical mastectomy, with wildly different surgical techniques than what are used today.) According to the The American Society of Breast Surgeons, “use of the ipsilateral arm for IVs or blood pressures is not contraindicated”. Likewise, the Society for Ambulatory Anesthesia says “SAMBA supports the placement of intravenous catheters, venipunctures, and blood pressure measurements in an upper extremity ipsilateral to breast cancer surgery with and without axillary lymph node dissection.” Kudos to Josh (@reverendofdoubt) for pointing this paper out to me.
Bottom line: It is almost certainly fine to place an IV or draw blood from the ipsilateral arm after breast surgery. Be cognizant of the fears these patients might have, and the misinformation they might have received. Teaching and shared decision making may be required.
Trauma patients need salt water?
Crombie N, Doughty HA, Bishop JRB, Desai A, Dixon EF, Hancox JM, Herbert MJ, Leech C, Lewis SJ, Nash MR, Naumann DN, Slinn G, Smith H, Smith IM, Wale RK, Wilson A, Ives N, Perkins GD; RePHILL collaborative group. Resuscitation with blood products in patients with trauma-related haemorrhagic shock receiving prehospital care (RePHILL): a multicentre, open-label, randomised, controlled, phase 3 trial. Lancet Haematol. 2022 Apr;9(4):e250-e261. doi: 10.1016/S2352-3026(22)00040-0. PMID: 35271808
This trial has a number of issues, which are going to be hard to describe in a brief paragraph. If you want the details, check out the full blog post. It is a multicenter RCT looking at fluid resuscitation in trauma patients, and comparing blood products to normal saline in the prehospital setting. The blood products group could receive a total of 2 units of PRBCs and 2 units of plasma. The saline group could have up to a liter of saline. Their primary outcome was the biggest problem with the trial: a composite of death and lactate clearance. One of those things is clearly not like the other, and they should never be combined into a single outcome. Luckily, it doesn’t seem to have mattered, as there were no differences at all. Mortality was 43% in the blood group and 45% in the saline group (p=0.57). Failure to clear lactate occurred in 50% of the blood group and 55% of the saline group (p=0.33). To some extent, I think these results will surprise some trauma people, as there has been a big push to replace blood with blood. However, I think if you pause and think about the study design for a minute, the results are not surprising at all. We are only talking about 1 liter of trial fluids in the prehospital arena. Even the most staunch supporters of blood products in trauma have never been all that bothered by 1 liter of normal saline. It is only when you start replacing 2-3 liters of blood with salty water that any of us get all that concerned, so I would have bet strongly on this trial having a negative outcome based solely on the protocol.
Bottom line: Using a small amount of blood over a small amount of saline in the prehospital setting did not affect outcomes in these trauma patients. However, in the emergency department, the appropriate fluid for hypotensive bleeding trauma patients is still going to be blood.
Some SHOCKING results
Schmidt AS, Lauridsen KG, Møller DS, Christensen PD, Dodt KK, Rickers H, Løfgren B, Albertsen AE. Anterior-Lateral Versus Anterior-Posterior Electrode Position for Cardioverting Atrial Fibrillation. Circulation. 2021 Dec 21;144(25):1995-2003. doi: 10.1161/CIRCULATIONAHA.121.056301. Epub 2021 Nov 24. PMID: 34814700
This paper surprised me. I have always heard that anterior-posterior pad position is the best for defibrillation and cardioversion. If anything, I would have thought a ‘myth busting’ paper might show no difference. However, this RCT concludes that the anterior-lateral position is significantly better. It is a multicenter open-label RCT in 468 elective outpatients with atrial fibrillation. For the primary outcome, anterior-lateral pad position was significantly better than anterior-posterior after the first shock. Success rate was 54% with anterior-lateral as compared to 33% with anterior-posterior, an absolute difference of 21% (95% CI 13-30%), and a number needed to treat of only 5. For what I think is the more important outcome, overall success rate, anterior-lateral was still better, with a success rate of 93% as compared to 85% with anterior-posterior (ARR 7%, 95%CI 2-12%, NNT 14). There are a number of problems with the trial, the biggest of which was that it was non-blinded. However, return to sinus rhythm is relatively objective, and their protocols were reasonably good, so I don’t know that the lack of blinding introduced all that much bias. It is also reasonable to ask whether elective cardiology patients will extrapolate well to emergency department patients. I expect our overall success rate might be higher, but I can’t think of any difference between these two populations that would influence the effectiveness of one pad position over the other.
Bottom line: I think this is strong enough evidence to favour the anterior-lateral pad position for cardioversion of afib in the ED.
Our biased brains, or “you are not as smart as you think you are”
Ly DP. The Influence of the Availability Heuristic on Physicians in the Emergency Department. Ann Emerg Med. 2021 Nov;78(5):650-657. doi: 10.1016/j.annemergmed.2021.06.012. Epub 2021 Aug 6. PMID: 34373141
This is a fascinating study, which uses an interesting before and after technique to demonstrate availability bias in the real world setting. (I liked the study enough that, despite its retrospective observational nature, I gave it a dedicated blog post, which can be found here.) Using a large VA hospital database, this study looks at individual physicians, and compares the 60 days before they made the diagnosis of a PE to the 60 days after, in day 10 increments. In the 10 days immediately after making the diagnosis of a PE, physicians were more likely to order tests for PEs (a 1.4% absolute increase or 15% relative increase). This returned to baseline in the subsequent 10 day period. Considering that there was nothing different about the patients in that 10 day period, this increase represents biased thinking on the behalf of the physician (everything looks like a PE when you just diagnosed a PE), and therefore represents pure harm to the patients. Although there are significant limitations to retrospective observational data, the design of this study means that those usual limitations are less likely to be at play. (Because they are comparing physicians to themselves, the data limitations should be the same before and after, and they are looking at objective orders in DDimers and CTPAs). Prior to this study, almost all research on cognitive bias in medical settings occurred in simulated vignettes. I think this is a very important publication, highlighting the importance of cognitives biases in medicine. Unfortunately, this study doesn’t provide us with what we really want: a way to avoid such errors.
Bottom line: This retrospective database study provides real world evidence that availability bias influences physician decision making, to the detriment of our patients.
Another study that says we are not as great as we think we are
Pappal RD, Roberts BW, Mohr NM, Ablordeppey E, Wessman BT, Drewry AM, Winkler W, Yan Y, Kollef MH, Avidan MS, Fuller BM. The ED-AWARENESS Study: A Prospective, Observational Cohort Study of Awareness With Paralysis in Mechanically Ventilated Patients Admitted From the Emergency Department. Ann Emerg Med. 2021 May;77(5):532-544. doi: 10.1016/j.annemergmed.2020.10.012 PMID: 33485698
This is a very concerning paper. It is a prospective observational trial from a single emergency department, in which all adult patients who were mechanically ventilated in the emergency department were contacted after they woke up (patients who didn’t wake up were excluded) to determine if they had any awareness while being paralyzed. Of the 383 patients included in the study, 10 (2.6%; 95% CI 1.3%-4.7%) were thought by their adjudication panel to have had awareness during paralysis. Use of rocuronium was strongly associated (OR 5.1) with awareness during paralysis. There are some obvious and significant limitations to this data. It is based on patient recall, and these patients would all have been altered, either by drugs or critical illness, so there is clearly a lot of subjectivity in this outcome. But the exact number probably doesn’t matter when it is an order of magnitude higher than the rate generally reported in the operating room. The other big drawback is that it is single-center data, which means that this hospital might just suck at post-intubation sedation. However, I think there is lots of other data to suggest we all suck, and this center is just brave enough to admit it in a major journal. Even with a lot of uncertainty about the exact number, I think this data tells us that awareness with paralysis is likely much more common in the emergency department setting than has been reported in the anesthesia literature. (This can be predicted from the anesthesia literature, because inhaled anesthesia is very protective, whereas IV only anesthesia in sick patients is associated with more awareness.) We all know this. We all have it drilled into us. And yet it continues to happen. I think that tells you that just relying on clinician memory will never be good enough, and we need systems based approaches to solve this issue.
Bottom line: The number of patients who are awake while paralyzed is probably much much higher than we would like in emergency medicine, and we need to fix that problem.
YEARS plus age adjusted Ddimer is best for PE
Freund Y, Chauvin A, Jimenez S, Philippon AL, Curac S, Fémy F, Gorlicki J, Chouihed T, Goulet H, Montassier E, Dumont M, Lozano Polo L, Le Borgne P, Khellaf M, Bouzid D, Raynal PA, Abdessaied N, Laribi S, Guenezan J, Ganansia O, Bloom B, Miró O, Cachanado M, Simon T. Effect of a Diagnostic Strategy Using an Elevated and Age-Adjusted D-Dimer Threshold on Thromboembolic Events in Emergency Department Patients With Suspected Pulmonary Embolism: A Randomized Clinical Trial. JAMA. 2021 Dec 7;326(21):2141-2149. doi: 10.1001/jama.2021.20750. PMID: 34874418
I spend a lot of time talking about how we need to test our tests with RCTs rather than just relying on observational data speaking to accuracy, so I was bound to love this trial. Over the last decade, testing for PE has increased dramatically, but so have the tools available to try to decrease testing. By now, I imagine most people are using age adjusted Ddimers, but the YEARS rule has been less widely implemented. This is a cluster-randomized, crossover, noninferiority trial at 18 emergency departments in Spain and France. The excluded patients who were PERC negative, as well as those with a high probability of PE, which they defined as greater than 50%. For everyone else, patients either used a YEARS algorithm with an age adjusted DDimer, or just an age adjusted DDimer. (This is different from the original YEARS derivation, which didn’t use an age adjusted DDimer. That being said, I think it reflects real life practice. If you fail YEARS, I just revert to my usual strategy, which is the use of an age adjusted DDimer.) Randomization was done at department level, so each ED stuck with one strategy.
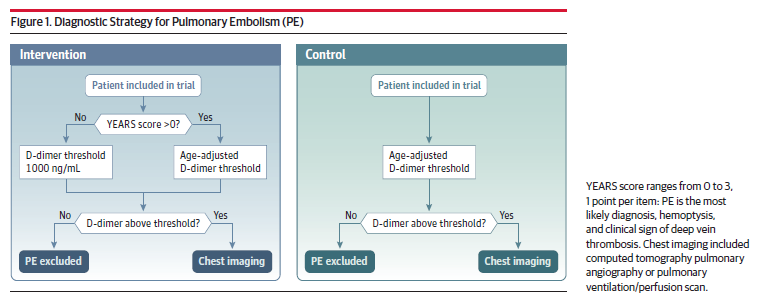
Their primary outcome was failure of the diagnostic algorithm, defined as a venous thromboembolism diagnosed within 3 months after being ruled out on the first visit. They randomized 1414 patients, of which 1271 were included in the per-protocol analysis. (Because it is biased towards a bigger difference between the groups, the per-protocol analysis is favored in non-inferiority trials.) There were a total of 6 PEs diagnosed in the 3 months after discharge. There was 1 miss (0.15%) in the YEARS group and 5 misses (0.86%) in the age-adjusted group. Obviously both of these miss rates are perfectly acceptable. The difference was noninferior, but the YEARS group was not that far off from being superior. The YEARS group also resulted in less chest imaging overall (30% versus 40%). This looks like a clear win for this modified YEARS algorithm, and although we will probably see more research in the future, I think this cluster RCT data is strong enough to implement the algorithm right now.
Bottom line: The combined YEARS and age adjusted DDimer outperformed the age adjusted DDimer alone in this trial.
Screening almost never works
Jiménez D, Agustí A, Tabernero E, Jara-Palomares L, Hernando A, Ruiz-Artacho P, Pérez-Peñate G, Rivas-Guerrero A, Rodríguez-Nieto MJ, Ballaz A, Agüero R, Jiménez S, Calle-Rubio M, López-Reyes R, Marcos-Rodríguez P, Barrios D, Rodríguez C, Muriel A, Bertoletti L, Couturaud F, Huisman M, Lobo JL, Yusen RD, Bikdeli B, Monreal M, Otero R; SLICE Trial Group. Effect of a Pulmonary Embolism Diagnostic Strategy on Clinical Outcomes in Patients Hospitalized for COPD Exacerbation: A Randomized Clinical Trial. JAMA. 2021 Oct 5;326(13):1277-1285. doi: 10.1001/jama.2021.14846. PMID: 34609451
If you look for PEs, you will find them. This is a consistent issue among inpatients with various presenting complaints. If you go looking for PEs in patients being admitted for COPD, somewhere between 6% and 20% of patients will have PEs identified. The same is true of syncope patients. The question is whether finding these PEs actually helps patients. (The next paper discusses this problem in more depth). Finally, rather than just arguing about this theoretically, we have an RCT to guide us. This is a multi-center RCT of 746 adult patients being admitted to hospital for a COPD exacerbation, and they were randomized to either get a routine workup for PE or just usual care. The DDimer was positive in half of the patients tested, and ultimately 16 PEs were identified on CTPA among the 369 randomized to get a PE work up. (A rule in rate of 4%, which is lower than other studies, but still above most calculations of the PE test threshold). In the control group, only 5 of the 367 patients underwent a PE workup, and 3 of these patients had PEs. Despite finding all these extra PEs with routine workups, there was no difference in their composite primary outcome looking for potential consequences of missed PEs at 90 days (29% in both groups). The rate of VTE diagnosed in the next 3 months was not statistically different, but was a little higher in the control group (0.5% vs 2.5%). Mortality was also not changed (6.2% vs 7.9%). Although there are some issues with this trial, and it really should be replicated, it represents the best evidence we have on the topic to date. This data suggests that routinely screening admitted COPD patients doesn’t provide clinical benefit, and that most of the PEs found represent overdiagnosis. (The same is almost certainly true of COVID patients.) That being said, you should still work up patients in whom you think PE is the primary cause, and these results may not apply to higher risk populations.
Bottom line: Routinely assessing admitted COPD patients for PE doesn’t provide any clinical benefit.
And that brings us to: overdiagnosis
Vigna M, Vigna C, Lang ES. Overdiagnosis in the emergency department: a sharper focus. Intern Emerg Med. 2022 Mar 5. doi: 10.1007/s11739-022-02952-8. Epub ahead of print. PMID: 35249191
This is a fantastic article, which I think I will add to my ‘must read’ list for emergency physicians. It discusses the topic of overdiagnosis, which occurs when an individual is assigned a diagnostic label that will never help them, and only result in harm. This is an essential consideration whenever making a diagnosis, and seeing as emergency medicine is primarily a diagnostic specialty, overdiagnosis should always be on our minds. This paper discusses some of the systemic issues that drive overdiagnosis in modern medicine (medical education, funding models, research agendas, liability concerns, patient expectations, and physician expectations). It then discussed 4 common examples of overdiagnosis in medicine. I have discussed pulmonary embolism, stress testing in CAD, and aneurysms in the workup of SAH many times before on the blog. I have to admit, the idea that anaphylaxis could be overdiagnosed (and therefore a harmful label) sort of blew my mind a little. I have a full blog post on this paper, but I truly think this is a paper that everyone should take the time to read.
Diverticulitis: time to change practice
Mora-López L, Ruiz-Edo N, Estrada-Ferrer O, Piñana-Campón ML, Labró-Ciurans M, Escuder-Perez J, Sales-Mallafré R, Rebasa-Cladera P, Navarro-Soto S, Serra-Aracil X; DINAMO-study Group. Efficacy and Safety of Nonantibiotic Outpatient Treatment in Mild Acute Diverticulitis (DINAMO-study): A Multicentre, Randomised, Open-label, Noninferiority Trial. Ann Surg. 2021 Nov 1;274(5):e435-e442. doi: 10.1097/SLA.0000000000005031. PMID: 34183510
This is at least the 4th RCT we’ve covered on antibiotics for diverticulitis, and they all say the same thing: antibiotics don’t help. I think it’s time to change your practice. This is a multi-center, open-label, noninferiority RCT that compared amoxicillin/clavulanate (875/125mg q8h) plus symptomatic therapy to symptomatic therapy alone in adults with uncomplicated acute diverticulitis on CT. They excluded sicker patients, such as uncontrolled diabetes and patients with any form of immunosuppression. Unlike some of the prior studies, patients were all treated as outpatients, which helps make the data applicable, although the follow-up was far more intense than most of us have access to. They enrolled 480 patients, and there was no difference in the number of patients requiring admission to hospital after a revisit to the ED (their primary outcome): 5.8% in the antibiotic group and 3.3% in the no antibiotic group, 2.5% absolute difference, 95% CI 6.32 to -1.17%). This was well within their non-inferiority limit, but their non-inferiority limit was set way too big in my opinion. (More on the massive problems with non-inferiority trials in a future blog post). The secondary outcomes were all very similar in both groups as well. This one trial alone may not be enough to change your practice, given the open-label non-inferiority design, but there is plenty of evidence that all says the same thing. If you are too much of a wimp to follow the evidence, you could ease into this practice by offering patients with uncomplicated diverticulitis a delayed antibiotics prescription, even though I usually think delayed antibiotics are dumb.
Bottom line: I can understand ignoring the first couple RCTs that go against such an ingrained practice, but this is at least the 4th such study, and there isn’t any evidence that antibiotics help. I think it is clearly time to change practice.
A not too long summary of long COVID
Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med. 2022 Mar;28(3):583-590. doi: 10.1038/s41591-022-01689-3. Epub 2022 Feb 7. PMID: 35132265
I have not spent a lot of time reading or talking about long COVID. In large part, this is because the science of this new entity is so shaky, and it is so difficult to distinguish between physical and psychological symptoms. However, over the last month or so, at least 10% of the patients I am seeing in the emergency department are presenting with symptoms that could be attributed to long COVID, so it is probably time to start throwing some papers in here. This is a massive cohort study that makes use of the Veterans Affairs database in the US. They compare 153,760 patients more than 30 days from their confirmed COVID infection, to 5,637,647 contemporary controls who did not have evidence of COVID infection (as far as the database could tell), and another 5,859,411 controls from 2017 who could not have possibly had COVID. They looked at outcomes over the course of 1 year, and the patients with a history of COVID had higher rates of essentially everything. A COVID diagnosis was associated with increased risk of stroke (HR 1.52), TIA (HR 1.49), atrial fibrillation (HR 1.71), ventricular dysrhythmias (HR 1.84), cardiac arrest (HR 2.45), pericarditis (HR 1.85), myocarditis (HR 5.38), myocardial infarction (HR 1.63), heart failure (HR 1.72), pulmonary embolism (HR 2.93), and DVT (HR 2.09). All of these outcomes were highly statistically significant, but with a database of millions, almost any finding, even if clinically insignificant, would be statistically significant. This study does not separate out vaccinated from unvaccinated COVID infections, so it cannot tell us if vaccination mitigates this apparent risk. There are obviously significant limitations anytime that a database is used to generate information. Aside from simple issues of misclassification, people who had recently been diagnosed with COVID probably have more visits with their primary doctors, resulting in more tests, some of which may be unnecessary. It is quite possible that a large component of this excess risk is the result of overdiagnosis or false positive tests, such as the notoriously unreliable stress tests.There is one sensitivity analysis that they don’t include: a comparison to a group of patients with a different infectious disease, such as influenza. Inflammation has long been tied to cardiovascular outcomes, so what I really want to know is how much extra risk COVID presents. An even bigger issue is what we are supposed to do with this information as emergency doctors. It’s not like we can go back in time and eliminate COVID, and it is very clear that in most jurisdictions, politicians have decided to completely ignore medical expertise, so it’s not like we even have very much power to limit the spread of COVID-19. We have essentially all been relegated to the classic scientist in a disaster movie role: forced to watch the disaster unfold, as incomptent people in positions of power make hopelessly bad decisions.
Bottom line: There is clearly a lot we don’t know about the long term implications of COVID-19. We should still be doing everything in our power to ensure that as few people as possible are infected by this virus.
Nailed it
Blereau C, Radloff S, Grisham J. Up in Flames: The Safety of Electrocautery Trephination of Subungual Hematomas with Acrylic Nails. West J Emerg Med. 2022 Feb 23;23(2):183-185. doi: 10.5811/westjem.2021.10.53567. PMID: 35302451
This paper offers an interesting warning that, if you are anything like me, you probably hadn’t considered. Acrylic is flammable. Many people have acrylic nails. As a treatment for subungual hematoma, many people use hot electrocautery as their trephination tool of choice. See the problem? In this fun little study, they put acrylic nails on 200 fake fingers, and then trephinated them using disposable electrocautery pens to see what happens. 83 times (42%) the nail caught fire. Not something you want to discover for the very first time with a patient. (Personally, I find that the electrocautery scares patients and the smoke is unpleasant. For trephination, I just use an 18 gauge needle using a gentle drill like rotation. It takes a little extra time – 1-2 minutes for a couple holes – but thus far, it has been 100% successful, with no pain or complaints from my patients.)
Bottom line: Try not to light your patients on fire.
Cheesy Joke of the Month
It is a five minute walk from my house to the bar, but a 45 minute walk from the bar to my house.
The difference is staggering.



3 thoughts on “Research Roundup (May 2022)”
The post on the vitamin C study is just, wow. I have no words. I’d say “It’s not even good fraud” except obviously it was good enough that it was believed! And had many studies done to replicate it! I think we as consumers of the medical literature don’t think about the possibility of fraud enough. When we see a study that seems to good to be true we might think the authors did some p-hacking to make a poor study look better, but we don’t tend to think that the data might be outright fraudulent. Perhaps it is time we started.
I just wrapped up a small pilot study on delirium prevention, and while we randomized well on the baseline characteristics we chose for randomization, it turned out that cognitive function, which we tested for and was not part of randomization, was not evenly distributed among the four groups. I’ve been very frustrated with this. But! At least now I can rest assured that my paper is not fraudulent. If I was going to produce fraudulent data, I would have done a better job.
Thank you so much for your contribution Justin!
Always great to read the research roundups!
Cheers from Brazil!