One of the true values of evidence based medicine is that it provides you with a systematic approach to new questions; an approach that should provide the best possible answer. Just a few months ago, I had never even considered the difference between a droplet and an aerosol. Now, I may have read more papers on this topic than any other topic in medicine. The bulk of that reading is summarized in the post “Aerosols, Droplets, and Airborne Spread: Everything you could possibly want to know”. In that post, I include a section on the “2 meter rule”, and conclude that the best science suggests that droplets can easily travel further than 2 meters (the cutoff often used to ‘keep us safe’ from COVID-19). However, as much as I try to be thorough in my deep dive evidence reviews, I don’t employ the strict methodology required of a systematic review, so it is always possible that I have missed important papers. Therefore, although their conclusions are the same as mine, I think it is valuable to review this systematic review looking at the distance that droplets spread.
The paper
Bahl P, Doolan C, de Silva C, Chughtai AA, Bourouiba L, MacIntyre CR. Airborne or droplet precautions for health workers treating COVID-19? [published online ahead of print, 2020 Apr 16]. J Infect Dis. 2020;jiaa189. doi:10.1093/infdis/jiaa189 PMID: 32301491 [article]
The Methods
This is a systematic review to determine the distance travelled by respiratory droplets. They followed the PRISMA criteria, and searched all dates up to March 2020, but limited their search to English language publications. They included any study that examined the horizontal spread of droplets.
The Results
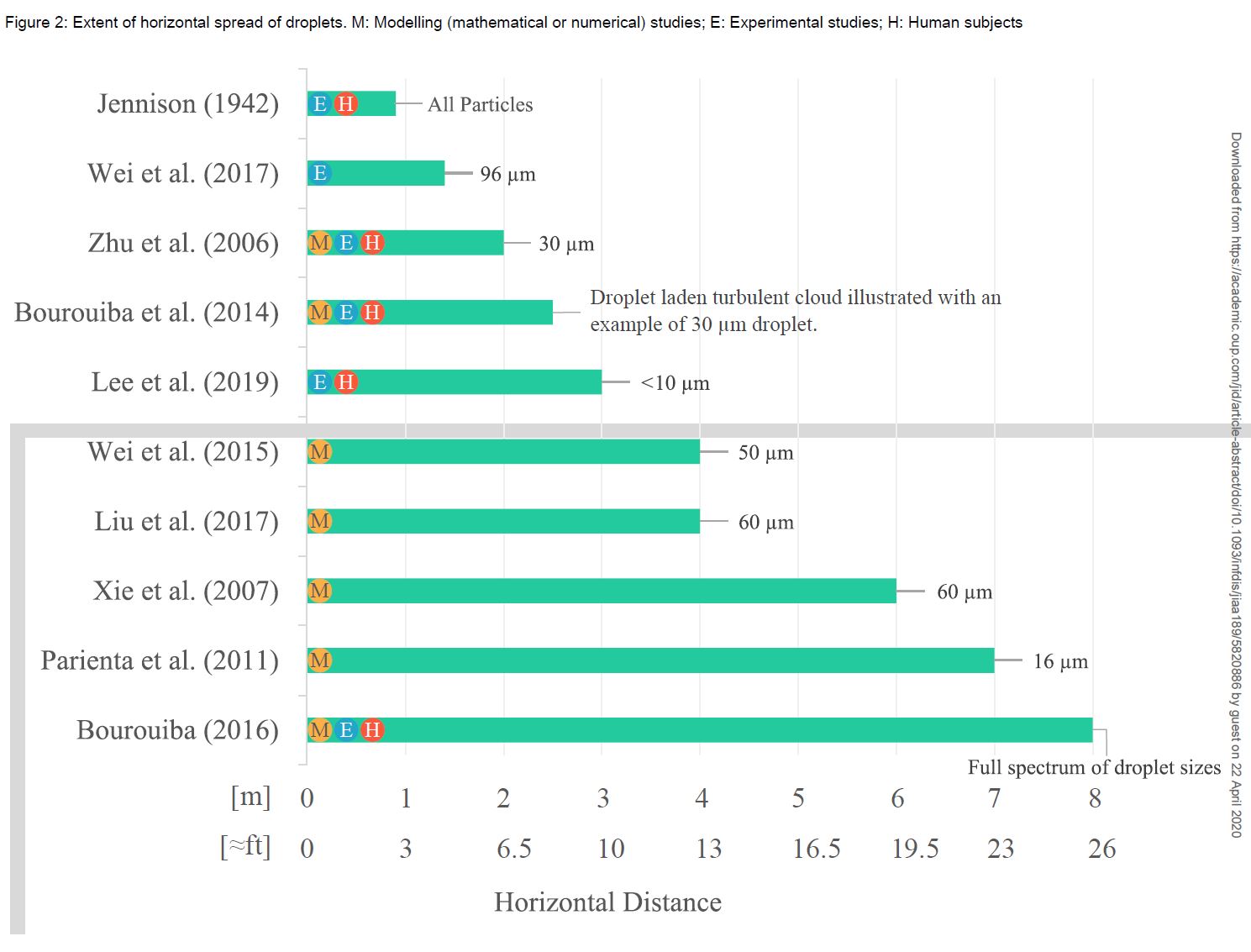
Out of 393 papers screened, 28 were selected for full text review, and 10 were included in the final analysis. As I discussed in the main aerosol and droplet post, most of these papers are based on modelling rather than empirical observation.
Eight of the 10 studies demonstrated a horizontal droplet trajectory of more than 2 meters. In the modelling studies, the range of horizontal spread was between 2 and 8 meters.
Two studies used water tank experiments to validate the models, and empirically demonstrated droplet spread between 1.4 and 2.5 meters.
There were 5 studies that included human participants, 4 of which used various cameras or detectors to observe natural coughs and sneezes, and 1 of which involved placing powder in a participant’s mouth (which could alter the natural spread of droplets). 4 of the 5 studies illustrated droplet spread beyond 2 meters. The only study that concluded that droplets don’t spread beyond 1 meter was published in 1942, and the authors of this review state that “no details were provided about how they reached this conclusion.”
My thoughts
The data here is far from perfect. For such an important topic, there is surprisingly little science. However, I think the available data makes it pretty clear that droplets will regularly travel beyond the 1 or 2 meter “safe zones” that we are currently using to protect healthcare staff. At very least, there doesn’t seem to be any scientific basis for the widely used 2 meter rule.
To quote the authors, “although the studies employed very different methodologies and should be interpreted cautiously, they still confirm that the spatial separation limit of 1 m (≈3 ft) prescribed for droplet precautions, and associated recommendations for staff at ports of entry, are not based on current scientific evidence.”
The biggest caveat to this data is that I don’t think any of the participants were wearing masks, which would significantly alter droplet distribution.
What is unclear is the importance of these droplets. What percentage of droplets make it beyond 2 meters, and how much virus do they carry? (The concentration of droplets drops rapidly with distance, as they are distributed through 3 dimensional space.) What is the absolute risk of viral transmission when standing at 2 meters, and what can I do to change it? How do the risks of taking PPE off 2 meters from the patient compare the the risks of carrying contaminated PPE further into the department? I don’t think we have clear answers to any of those questions.
The picture is further complicated by the existence of aerosols. This study focused on droplet spread, and doesn’t really tackle aerosols, which can remain airborne for much longer and travel far greater distances. (As I covered in my last post, aerosolized COVID-19 has been found in the air at least 4 meters away from patients.) (Guo 2020) These authors argue (as I did) that the distinction between aerosols and droplets is not black and white. There is reason to believe that COVID-19 can be spread through the airborne route, but it isn’t clear how big a risk airborne transmission represents. (Wilson 2020)
These authors make a strong argument for the precautionary principle. They note the heavy toll paid by healthcare workers during both SARS and MERS, and emerging evidence of a high rate of transmission to healthcare workers during COVID-19. They argue that, based on the viral load in both the upper and lower respiratory tracts, the virus’ viability in air beyond 3 hours, and recent studies demonstrating aerosol spread, that airborne transmission is possible. They note that both the CDC and WHO recommended N95 respirators for all clinical encounters with SARS patients. The CDC and the European CDC initially also recommended respirators for COVID-19 as well, but later changed their guidelines in the face of PPE shortages. However, although I agree that in an ideal world N95s would be used for all patient encounters, that is just not a practical suggestion, and could result in significant harm if masks are not available for high risk encounters because they were all used for very low risk encounters. Unfortunately, it still isn’t clear exactly which encounters are high and low risk.
Bottom line
Most of this data was included in the original write up, so my bottom line doesn’t change. There is no such thing as the “2 meter rule”. The further you are from the patient, the lower your risk of exposure to doplets. Getting behind a closed door should eliminate your risk completely.
However, you have to be careful about extrapolating this data too far. Everything in medicine has harms. Although this data indicates that you want to be as far as possible from the patient when taking off your PPE, the harm of spreading virus through clean working areas on contaminated PPE also has to be considered. How this data is applied will depend a great deal on the physical layout of your working space.
Other FOAMed
Aerosols, Droplets, and Airborne Spread: Everything you could possibly want to know
Depth of Anesthesia Podcast: Does covid-19 spread by aerosols and aerosol-generating procedures?
References
Bahl P, Doolan C, de Silva C, Chughtai AA, Bourouiba L, MacIntyre CR. Airborne or droplet precautions for health workers treating COVID-19? [published online ahead of print, 2020 Apr 16]. J Infect Dis. 2020;jiaa189. doi:10.1093/infdis/jiaa189 PMID: 32301491
Guo ZD, Wang ZY, Zhang SF, et al. Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020 [published online ahead of print, 2020 Apr 10]. Emerg Infect Dis. 2020;26(7):10.3201/eid2607.200885. doi:10.3201/eid2607.200885 PMID: 32275497
Wilson NM, Norton A, Young FP, Collins DW. Airborne transmission of severe acute respiratory syndrome coronavirus-2 to healthcare workers: a narrative review [published online ahead of print, 2020 Apr 20]. Anaesthesia. 2020;10.1111/anae.15093. doi:10.1111/anae.15093 PMID: 32311771
Morgenstern, J. Droplets spread more than 2 meters (a systematic review), First10EM, April 27, 2020. Available at:
https://doi.org/10.51684/FIRS.18655

2 thoughts on “Droplets spread more than 2 meters (a systematic review)”