A key scientific lesson that I have discussed numerous times on this blog is that the interpretation of any new study must be placed within the context of what is already known about the topic. Although there must be equipoise for medical research to be ethical, equipoise does not mean that every trial has a 50% chance of succeeding. (In fact, the vast majority of novel interventions fail in medicine). Some therapies are much more likely to succeed than others, and that pretest probability is important when interpreting a new trial. For example, if I have 2 identical trials with p values of 0.04, but one looked at aspirin and the other at homeopathy, I am much more likely to believe the results of the aspirin trial. The last few years have seen a number of controversial trials involving tranexamic acid (TXA). WOMAN and CRASH-3 were both negative trials, but with potentially interesting secondary analyses that resulted in them being widely advertised as positive. What you make of those secondary analyses will depend a lot on how much you believe in TXA in general. After CRASH-2, TXA was hailed as a wonder drug, but does it deserve that reputation? In an effort to appropriately calibrate my pretest probability for CRASH-3 and WOMAN, I began the effort of reading and summarizing the literature on TXA for essentially every indication, and this blog post is the culmination of that effort.
Very Basic Physiology
Tranexamic acid reversibly attaches to plasminogen, preventing its activation to plasmin, thus preventing the breakdown of fibrin clots. It is also a competitive inhibitor of tissue plasminogen activator (tPa). Plasmin is also involved in a number of inflammatory cascades, which explains why TXA has also been suggested as a therapy for angioedema. (Morison 2013; Hunt 2015)
(Did you know that Tranexamic acid is actually still a short form? It’s real name is trans-4-(aminomethyl) cyclohexanecarboxylic acid.) Personally, I will stick with TXA.
TXA for Surgery
Bottom line: Although there are a huge number of studies, the actual benefit is unclear. There is a consistent signal that perioperative blood loss is reduced. However, blood loss is a surrogate outcome, and its measurement can be somewhat subjective. Furthermore, most these RCTs are tiny (the largest have about 100 patients per group and many have 10-20), which reduces overall quality, and means we are very unlikely to see possible harms. Ultimately, it is impossible to know whether there is a net patient oriented benefit.
There are a huge number of studies (252 RCTs) looking at antifibrinolytics to reduce perioperative blood loss, and the total number of patients included seems very large (more than 25,000), but the individual studies are all still very small, with a significant risk of bias, and in particular evidence of publication bias. (Henry 2011) Focusing specifically on TXA, the Cochrane review found 65 trials which included 4842 patients comparing TXA to a control. TXA reduced the need for blood transfusion by 18% (RR 0.61, 95% CI 0.53-0.7). TXA did not reduce the total volume of blood being transfused (0.3 units less in the TXA group, 95% CI 0.8 units less to 0.1 units more). Post-operative blood loss was reduced by an average of 247 mL (95% CI 200-295). There was no difference in mortality, reoperation for bleeding, MI, stroke, DVT, or PE. (Henry 2011)
However, the funnel plots show pretty clear evidence of publication bias. (The higher quality, larger studies all cluster around no effect. The lower quality, smaller studies essentially all favour TXA. Thus, there were almost certainly many lower quality negative studies that never got published.) There is also concern about under-reporting of adverse events in these smaller trials.

I will never have time to read all of these individual RCTs. However, there are problems with the few I have picked up. For example, although Aremellin (2001) is a double-blind RCT with a reasonable size, they retrospectively excluded a number of patients who seem pretty important to the trial, including patients who needed a re-exploration of their wound for post-operative blood loss. Excluding select patients who are bleeding from a trial looking at bleeding after randomization is a big red flag and major potential source of bias.
The single biggest trial is the ATACAS trial: a multi-centre RCT comparing TXA to placebo (although many patients were unblinded) in 4662 patients undergoing elective coronary artery surgery. (Myles 2017) The primary outcome – a composite of death and thrombotic events within 30 days – was unchanged, occurring in 16.7% of the TXA group and 18.1% of the placebo group (p=0.22). In terms of secondary outcomes, there were improvements in the rate of return to the OR (1.4% vs 2.8%) and blood products administered (38% vs 56%), but TXA increased seizures (0.1% vs 0.7%). These are relatively small changes in disease oriented outcomes found on secondary analyses and are therefore of questionable relevance.
A Cochrane review focused specifically on emergent or urgent surgery identified 5 trials including a total of 372 patients. Again, TXA reduced the probability of getting a blood transfusion (RR 0.70, 95% CI 0.52-0.94), but there was no impact on mortality (RR 1.01, 95% CI 0.14-7.3). The point estimate for DVT (RR 2.29) and stroke (RR 2.79) were both concerning, but the confidence intervals were huge. (Perel 2013)
These trials are small and the risk of bias is high. When combined with the high probability of publication bias, I think it is uncertain whether TXA even decreases blood loss, despite it being a relatively consistent finding. That is probably a moot point considering that there is no difference in any of the patient oriented outcomes. I think there is enough here to support a hypothesis that TXA decreases perioperative blood loss, but I think higher quality RCTs would be required to prove that hypothesis. Even if that hypothesis is confirmed, we will still need to see high quality studies that demonstrate that a decrease in blood loss actually translates into a patient important benefit that outweighs harms.
It is worth noting that aprotinin looks better than TXA across the board for all the surrogate outcomes that we get excited about (patients bleed less), but has been pulled from the market because of concerns that it increases mortality. (Henry 2011) This is a great reminder that we need to be very cautious when using surrogate outcomes.
TXA in surgery FOAMed: The Bottom Line ATACS trial
TXA for GI Bleeds
As an illustration of exactly how long I have been working on this post, this section was written well before the HALT-IT trial was published. I am leaving the original as an example of how science and scientific thought progresses. However, the HALT-IT trial, which is discussed at the end, demonstrates pretty clearly that TXA does not help in GI bleeding and supersedes all of these trials.
Original bottom line: Small trials with high risk of bias leave us unsure. The Cochrane review says “this review found no evidence that tranexamic acid offers benefit to patients with upper gastrointestinal bleeding, in terms of mortality, bleeding, surgery, or transfusion requirements.” However, their results do show a statistical significant reduction in mortality before their adjustments. (Bennett 2014) Hopefully the large RCT currently underway (HALT-IT) will settle the issue.
As of the 2014 Cochrane review, there were 8 RCTs including a total of 851 patients. (Bennett 2014) The results are promising, but the data is at high risk of bias, with small trials, and a high rate of attrition. There was a statistically significant reduction in mortality (RR 0.6, 95% CI 0.42-0.87), however that difference disappears when they try to account for the large number of lost patients. Also, there appears to be one trial that is a bit of an outlier (discussed below) because of the high rate of mortality in the control group, and this trial accounts for half of the patients in this analysis. The need for surgery was also statistically significant, but not after they adjusted for lost patients. The rebleeding number is in the right direction, but not statistically significant (RR 0.72, 95% CI 0.5-1.03). There was no difference in transfusion (RR 1.02 95% CI 0.94-1.11). The number of patients with thrombotic events was higher, but not statistically significant (RR 1.86, 95% CI 0.66-5.24).
The RCT by Barer (1983) is the largest single trial, with 775 patients, and makes up the majority of that Cochrane review. They randomized patients to either cimetidine, TXA, or placebo. All patients got the medications intravenously for 2 days and then orally for 5 days. The IV solutions were all identical, but the pills looked different, limiting that value of the initial blinding. They don’t state a primary outcome, but the trial was powered for the rate of operation. There was no change in the rate of operation or rebleeding. They do, however, note a decrease in mortality (6.3% with TXA vs 13.5% with placebo, p=0.009). Although that would clearly be an important outcome, there are a few concerns. It seems like it was a secondary outcome in a trial with a negative primary outcome. The authors admit that there is limited biologic plausibility to a decrease in mortality when TXA didn’t change either the amount of bleeding, nor the need for surgery. Finally, the rate of death in the placebo group is a lot higher than we see in other trials (usually around 5%). (Daneshmend 1992) Furthermore, I tend to be a little cautious about using evidence that was collected before I was born. (This is both because the quality of the science has changed with time, and also because our treatments have changed significantly. For example, endoscopic therapy was not routinely employed for upper GI bleeding in the early 1980s, so it is hard to know how these results would apply today.) We really need to see this mortality benefit repeated in another RCT.
There is a more recent RCT that looked at the use of topical TXA (through an NG tube) in upper GI bleed. (Karadas 2020) They excluded 5 patients after randomization because they had variceal bleeds, but this is a methodologic faux-pas. (We would obviously have to treat these patients in the ED, as we don’t know the source of bleeding, so their outcomes need to be considered as well.) The primary outcome is a pretty bad composite that includes things that really matter (mortality) with relatively irrelevant outcomes (ED revist). There was no statistically significant difference in this primary outcome, although the TXA group actually did worse (32.1% vs 29.1%, p=0.69). There were no statistically significant differences in anything. In terms of the most important outcome, mortality was 10.3% with TXA and 12.7% with placebo (p=0.64). This could represent a clinically important difference that the trial was simply not powered to detect.
The TAUGIB study was supposed to be finished in 2015, but it hasn’t been published and the results aren’t available anywhere. The HALT-IT trial is a large RCT currently underway to determine if TXA decreases all cause mortality. (Roberts 2014)
In the context of our current management of upper GI bleeds, I find this data fascinating. The data here is far stronger than that data we have for PPIs in undifferentiated GI bleeds (which actually suggests PPIs harm our patients), and yet no one uses TXA and everyone rushes to get a PPI infusion started. This data is weak, and I wouldn’t be surprised if the HALT-IT trial is negative, but if you had to choose between a PPI and TXA, I think TXA is clearly the better bet. That being said, it is likely that TXA will also turn out to be useless, and we really just need to focus on getting these patients to endoscopy for definitive therapy.
2020 Update: Of course, now the HALT-IT trial has been published, and my suspicions were confirmed: there is no benefit from TXA in GI bleeding. There is an in-depth summary of that trial here, but the quick summary is that HALT-IT is a large multicenter RCT which enrolled 12,009 adult patients with GI bleeding (90% had upper GI bleeds) and randomized them to either TXA or placebo. There was no change in all cause mortality, death due to bleeding, rebleeding, surgery, endoscopy, need for transfusion, or total blood products transfused. The only difference was an increase in venous thromboembolic events (from 0.4% to 0.8%).
Current Bottom Line: The best available evidence suggests that TXA should not be used in patients with GI bleeds, as it results in a small net increase in harm in the form of venous thromboembolism.
TXA in GI bleed FOAMed: TheNNT
HALT-IT FOAMed: First10EM, SGEM, St. Emlyn’s, REBEL EM, The Bottom Line
TXA for Postpartum Hemorrhage
Bottom line: We have 2 big trials that are negative, but there were some potential hints of an effect. The current best evidence is that TXA does not help in postpartum hemorrhage, but the secondary outcomes deserve follow up trials. TXA should not be given routinely, but I wouldn’t fault you if you decided to give it in a massive hemorrhage scenario.
Of course, the big trial here was the WOMAN trial. This was a massive RCT of 20,060 women worldwide with postpartum hemorrhage, randomized to either TXA or placebo. There was no difference in the primary outcome of all cause mortality or hysterectomy (5.3% vs 5.5%, RR 0.97, 95% CI 0.87-1.09). All cause mortality was also completely unchanged (2.3% vs 2.6%). There was some excitement about the secondary outcome of “death due to bleeding”, but as I explain in this post, disease specific mortality is a very poor outcome, that is both error prone and clinically irrelevant (especially when there is no change in all cause mortality). It is possible that this trial looked at the wrong population, but overall it is a pretty definitively negative trial, suggesting that TXA shouldn’t be used routinely in postpartum hemorrhage. (WOMAN collaborators 2017)
There are a few other small trials, but they don’t really add much to the issue. Ducloy-Bouthors et al (2011) performed an open label RCT of high dose TXA (4 grams over 1 hour, then 1 gram an hour for 6 hours) in 144 women with PPH and more than 800 mL of blood loss. The trial was statistically positive, but the actual outcomes were not impressive, with only a 48 mL difference in total blood loss between the groups. Ayedi et al (2011) randomized 51 patients with postpartum hemorrhage that continued despite oxytocin to TXA or placebo. (The study is only available as an abstract.) There were no deaths. There was a 600 mL difference in blood loss between the groups, but the result wasn’t statistically significant. Another small trial demonstrated no difference between TXA and misoprostol (Sahar 2014) although the evidence for misoprostol is also somewhat imperfect.
There is one other large trial worth considering, this time looking at TXA for the prevention of PPH. The TRAAP trial randomized 3891 low risk women after vaginal delivery to either 1 gram of TXA pushed over a minute or placebo. (Unlike other trials, there was no second dose of TXA, which could have disadvantaged the TXA group.) There was no difference in the primary outcome of blood loss of at least 500 mL (8.1% vs 9.8%, p=0.07, RR 0.83; 95% CI 0.68-1.01). They powered the study for an optimistic 30% reduction, but only saw 20%, so the study may be underpowered for a difference that could still be clinically significant. There were a few secondary outcomes that were statistically significant in favour of TXA. However, there were no differences in anything that looks clinically important (total blood loss 220 vs 236 mL; blood transfusion 0.9% vs 0.9%; need for surgery or embolization 0.2% vs 0.3%). The post delivery hemoglobins were also identical between the two groups, so the trial looks negative for everything that matters. (Sentilhes 2018)
The same group looked at TXA for the prevention of PPH after C-section in the TRAAP 2 trial. (Senthilies 2021) This time, they are able to report a positive primary outcome, but I actually think the trial is pretty negative. It is an RCT of 1 gram of TXA versus placebo in 4551 women. Their primary outcome was either an estimated blood loss greater than 1,000 mL or blood transfusion within 2 days of delivery (so disease rather than patient oriented). This outcome favoured TXA, occurring in 27% of the TXA group and 32% of the placebo group (p=0.003 with multiple imputation of missing values). However, nothing important changed at all. The measured difference in blood loss between the groups was only 30 mL – clinically irrelevant. There was no difference in the number of women needing transufions (1.6% vs 1.4%), the amount transfused (3.1 vs 3.2 units), clinically significant PPH as assessed by the doctor, ICU use, follow up hemoglobin, or need for invasive procedures. They don’t mention mortality anywhere in the manuscript, so I assume no one died. There was more nausea and vomiting with TXA (43% vs 36%, p<0.001). Clotting, although not statistically significant, does look a touch higher with TXA (0.4% versus 0.1%, p=0.08). Overall: nothing important changed, and so this is definitely not a selling point for TXA.
WOMAN FOAMed: First10EM, REBEL EM, SGEM, TheNNT
TXA for Nontraumatic ICH
Bottom line: The quality of evidence here is stronger than a lot of other areas, and the trials are clearly negative. At this point, there doesn’t seem to be any role for TXA in nontraumatic ICH.
The TICH 2 trial was a multi-centre, double-blind, randomised, placebo-controlled trial that randomized 2325 patients with non-traumatic intracranial hemorrhage to either intravenous TXA or placebo. Looking at functional outcomes at 3 months, there were no differences. The number of patients with a bad outcome (mRs >3) was 71% vs 72%. There was no difference in mortality. There was a statistical difference in hematoma size, but it was clearly clinically irrelevant (3.7 mL vs 4.9 mL). The biggest caveat with this trial is that it is possible that enrolling patients up to 8 hours is too long, and by then the damage is done. However, it is worth noting that the outcomes actually look better in the group of patients given TXA after 3 hours. (Sprigg 2018)
A Cochrane review found 10 RCTs, encompassing 1904 patients, looking at TXA for subarachnoid hemorrhage. (Baharoglu 2013) The overall quality isn’t great, with only 6 using placebo and only 5 employing an intention to treat analysis. TXA did not change the number of people with a poor neurologic outcome (RR 1.02, 95% CI 0.91 – 1.15). It also didn’t change all cause mortality (RR 1.00, 95% CI 0.85 – 1.18). There was a significant reduction in the rate of rebleeding (RR 0.64), however this was balanced by a significant increase in cerebral ischemia (RR 1.41). Neither surrogate really matters if both mortality and neurologic outcomes are completely unchanged.
Since then, there has been a much larger RCT looking at TXA in SAH. (Post 2021) It is a multi-center, open-label RCT that randomized patients to TXA or usual care as soon as a subarachnoid hemorrhage was identified. There was no difference in the primary outcome (good neurologic outcome), nor any of the secondary outcomes, although overall the outcomes look a little bit worse with TXA. The article has its own blog post.
Of note, I have seen numerous statements that TXA is contraindicated in SAH because of increased cerebral edema and infarction, but I haven’t actually found the data that these statements are based on. (Chan 2013)
TICH 2 FOAMed: First10EM, EM Lit of Note, SGEM, REBEL EM
TXA for Epistaxis
The initial summary for epistaxis was written before the NoPAC trial was published. (Reuben 2021) This was the initial bottom line: The level of evidence is weak, and so I wouldn’t be surprised if it was overturned in the future, but the current evidence does support the use of TXA (either topical or oral) to reduce the risk of rebleeding. There is no evidence that it reduces more important outcomes like transfusions or need for interventions or surgery.
NoPAC was that high quality RCT. So now the bottom line is: The best available evidence suggests that TXA does not provide any benefit in epistaxis, although the studies are still small and there could be a small unseen benefit. TXA is certainly not a miracle cure for epistaxis.
Prior to NoPAC, there were six RCTs which included a total of 692 patients. They had fairly different methods. Some used oral TXA and others used topical. The treatments in the control groups vary wildly. The Cochrane review rates the quality of these studies as “moderate to low”. (Joseph 2018)
One single-center, open-label RCT compared 500 mg of TXA on a cotton ball to usual packing in 216 patients with epistaxis. It worked quickly (bleeding was stopped at 10 min in 70% of the TXA group compared to only 30% of the packing group). Rebleeding at 24 hours was not statistically significant, but was lower in the TXA group (5% vs 10%). (Zahed 2013)
There is another non-blind, single-center RCT from the same group randomizing 124 adult patients taking antiplatelet medications with ongoing epistaxis after 20 minutes of pressure to either 500 mg of TXA on a cotton pledget or nasal packing with epinephrine and lidocaine. The results were remarkably similar, with 73% of the TXA groups having their bleeding stopped at 10 minutes as compared to 29% of the packing group. There was no difference in rebleeding at 24 hours (5% vs 10%), but this time it became statistically significant by 1 week (5% vs 21%). Patients also left the ED quicker in the TXA group.
The big concerns with these two studies are the lack of blinding and the fact that both these studies come from a single center. A third very similar study compared 1 gram of topical TXA to phenylephrine in 120 patients, and appears to have very similar results, but is not available in English so I can’t review it in detail. (Atabaki 2017)
Two inpatient studies looked at oral TXA (1 gram TID) compared to placebo. I don’t have access to Petruson (1974), and the trial isn’t listed on PubMed, but in admitted patients, all of whom had a Foley catheter and an anterior pack, oral TXA apparently resulted in a statistically significant decrease in rebleeding when the packs were removed. On the other hand, White (1988) looked at 89 admitted adult patients, and there was no statistical difference in the amount of rebleeding (57% with placebo, 47% with TXA). There was no difference in transfusion. They did find a statistical difference in the number of patients with minor rebleeds, but that means that there was absolutely no difference in the more important group of patients with major rebleeds.
Overall, TXA seems to reduce the rate of re-bleeding (47% vs 67%; RR 0.71, 95% CI 0.56-0.9). It isn’t clear whether it affects other important outcomes. The only study that reported transfusion rates showed no difference, and none of the studies reported how many patients required further interventions like surgery or repacking. Furthermore, these studies likely don’t provide us with an adequate representation of harms. The Cochrane review states that “the body of evidence included in this review (six studies with a total of 692 participants) is insufficient to allow robust conclusions to be drawn.” (Joseph 2018)
The NoPAC trail got its own write up. The quick summary is that it was a multi-center, double-blind RCT that included 496 adult patients with epistaxis who had already failed basic first aid measures. There was no difference in the primary outcome of need for anterior packing (43.7% of the TXA group were packed as compared to 41.3% of the placebo group), nor were there differences in any of the secondary outcomes. The trial is certainly not definitive, but is much stronger than anything available to date.
There are a few ongoing trials. NCT02930941 is an American single centre RCT of atomized nasal TXA or placebo looking to enroll 70 ED patients. It is supposed to be done in December 2019, but the results are not available yet. NCT03360045 is an RCT comparing topical TXA with Merocel packing in 135 ED patients in Turkey. The trial was apparently finished in August 2018, but the results are not available yet. (Academics is slow, but these delays increase the risk of publication bias.)
TXA in epistaxis FOAMed: First10EM, REBEL EM, TheNNT, St Emlyn’s, FOAM Cast
TXA for Tonsillectomy Bleeding
Bottom line: In a few small trials looking at the prevention of hemorrhage, the total amount of bleeding might have been decreased, but clinically important outcomes were not different.
As of 2013, there were 3 RCTs and 4 case control series looking at TXA for the prevention of post-tonsillectomy hemorrhage, with significant variation in the timing and dosage of TXA. (Chan 2013) These trials all focus on prevention, rather than the treatment of active bleeding, which would be of more interest in emergency medicine. TXA statistically reduced mean blood loss, but the total amount seems like it might be clinically insignificant (33 mL, 95% CI 23-43 mL). TXA did not reduce the risk of post-tonsillectomy hemorrhage (RR 0.51, 95% CI 0.25-1.07), but that is obviously a huge confidence interval, and most lies on the side of benefit. On the other hand, not all hemorrhage is significant, and the number of patients requiring further treatment was identical (RR 1.05, 95% CI 0.33-3.34), as was the mean fall in hemoglobin (0.9 vs 0.8 g/100mL)
TXA for Dental Bleeding
Bottom line: The evidence is very limited, and seems to suggest that TXA is not better than standard care.
There is a Cochrane review looking at the use of TXA to prevent oral bleeding after minor oral surgery in patients on anticoagulants. (Engelen 2018) There are no trials that look at TXA in the context of DOACs. There are 4 trials (3 RCTs) that look at TXA in patients with therapeutic INRs on warfarin. In the two trials that compared TXA to placebo (128 total patients), preventative topical TXA reduced the number of post-operative bleeds that needed an intervention. However, in the two trials that compared TXA to standard care (ie dry gauze compression), there was no difference. It is not surprising that there are some small positive studies, as that is par for the course with TXA. These studies date back to an era before trial registries, so publication bias becomes a big concern. More importantly, TXA doesn’t appear to perform any better than simple pressure with dry gauze. Unfortunately, these preventative studies don’t really help us in the emergency department, where we need to know how to deal with the patient who just won’t stop oozing blood at 3 in the morning. Unless I have missed something, there doesn’t seem to be any evidence to guide us there.
TXA for Hemoptysis
Bottom line: We don’t know. The trials are small and biased, but hint at some potential benefit. We clearly need a large RCT. What you do in the meantime will likely depend a lot on how you interpret the rest of the TXA literature.
There are 3 RCTs that look at TXA for hemoptysis. They are quite different, giving TXA for different lengths of time and using different routes of administration. None of the trials included sick patients with massive hemoptysis, so will be hard to extrapolate to the patients we care most about in the emergency department. There are some benefits reported, but they are inconsistent, and the trials are small. Importantly, the small number of trials suggests possible publication bias, considering the large number of trials for other indications. (Prutsky 2016)
One small (47 patients) RCT looked at nebulized TXA in non-massive hemoptysis and showed a significant improvement in the resolution of bleeding (96% vs 50%). The mortality numbers also look better, but aren’t statistically significant (0% vs 9%, p=0.21). However, there are a number of problems with the trial, including the fact that it was stopped early without any clear stopping criteria, the small numbers, some potentially important differences between the groups at baseline, and the fact that there are numerous simple math mistakes in the published manuscript. I don’t trust the results. (Wand 2018)
The two other trials are combined in a Cochrane review. (Prutsky 2016) One was a double-blind RCT comparing intravenous TXA (1 gram TID) to placebo in 24 inpatients with hemoptysis secondary to tuberculosis. (Ruiz 1994) The other is a double-blind RCT comparing oral TXA (500 mg TID) to placebo in 46 outpatients with hemoptysis from various causes. (Tscheikuna 2002) Overall, there was no difference in remission by 7 days (OR 1.56, 95% CI 0.44-5.46). Duration of bleeding was slightly shorter (mean difference 19 hours, 95% CI 12-27 hours). There were no serious adverse events in either study, but mild side effects (nausea, dizziness, vomiting, abdominal pain, and diarrhea) look higher with TXA (OR 3.13, 95% CI 0.8-12.24).
There is also a recent large retrospective study that used propensity matching to look at 9933 pairs of adult patients admitted to hospital for hemoptysis, comparing those who received TXA to those who didn’t. They report a mortality benefit (11.5% vs 9.0%), as well as a decrease in length of stay and decrease in cost. However, there were a large number of patients excluded without a clear reason, and this data is not randomized. With propensity matching, there is always a possibly missing important confounders. In this study they didn’t have access to vital signs, volume of hemoptysis, whether the patient was taking anticoagulants, or CXR findings, which are all pretty important factors in a study of hemoptysis. I don’t think this changes what we already knew: this topic needs a large RCT.
This is an indication where even a small decrease in bleeding could matter a lot. Therefore, I would expect a small decrease in total bleeding (the surrogate outcome) to be more likely to translate into true patient oriented outcomes than in something like GI bleeding or epistaxis. Whether TXA does in fact decrease bleeding remains to be seen.
TXA in hemoptysis FOAMed: First10EM, REBEL EM, EM PharmD
TXA for Hyphema
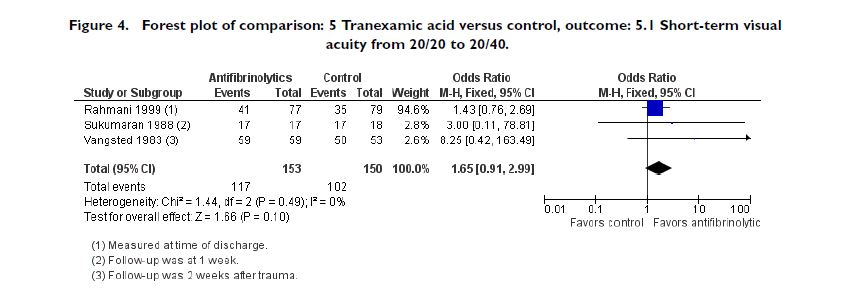
Bottom line: In a few small studies, TXA reduces rebleeding, but has no effect on visual acuity. The point estimates are on the right side, but the studies are just too small. We need a large RCT. In the meantime, the best answer is we don’t know.
The Cocharne review found 5 controlled studies including 581 patients that compared oral TXA to a control in hyphema. (Gharaibeh 2019) TXA reduces the risk of secondary hemorrhage (OR 0.25, 95% CI 0.13-0.49), however, it didn’t improve the primary outcome of visual acuity (OR 1.65, 95% CI 0.91-2.99). There is a concern about possible increased glaucoma (you don’t want solid blood clots staying in the anterior chamber), and the estimate was on the side of TXA being worse, but it wasn’t anywhere close to statistically significant (OR 1.23, 95% CI 0.7-2.16).
TXA for Dysfunctional Uterine Bleeding
Bottom line: The available evidence suggests a small benefit from TXA, but the available evidence is low quality.
The Cochrane review found 13 RCTs encompassing 1312 patients studying antifibrinolytics for dysfunctional uterine bleeding. (Bryant-Smith 2018) The overall quality of the studies was rated as very low and the studies were very small (average of 100 participants per study). Pooled, they found that TXA resulted in about a 50 mL decrease in total bleeding per cycle, and a significant improvement in the number of women who reported symptomatic improvement. However, half of the studies weren’t blinded, which really impacts such subjective outcomes. They didn’t report a difference in adverse events, but most of the studies didn’t even report on harms.
To me, this sounds a lot like the TXA research for other indications: small low quality studies suggest small improvements in disease oriented outcomes. (I have not had time to read the individual RCTs for DUB, so cannot comment on their individual quality aside from what is stated in the Cochrane review). However, for other indications, large high quality studies have pretty consistently contradicted the claimed benefits. My guess is that is what we will see here.
TXA for Post Circumcision Bleeding
One of my first EM:RAP pieces was on post-circumcision bleeding. The key take home message: the total blood volume of a neonate is a lot less than you think, so be very cautious. For that reason, I was interested in any evidence on the topic. Based on a literature search done by the BEST BETs team, there are no studies. (Madden 2021)
TXA for Trauma (including ICH)
For emergency medicine, trauma is where everything started. Around the time I was in residency, TXA went from a drug no one had ever heard of, to the magic bullet of our time. Hopefully, the evidence reviewed thus far has dispelled the magical bullet reputation, but what is the role of TXA in trauma?
Bottom line: Based on CRASH-2, the best evidence is that TXA reduces all cause mortality in bleeding trauma patients. However, science requires replication, and other sources of evidence are mixed, so the potential benefit of TXA in trauma should be viewed with a moderate degree of uncertainty.
Everyone knows about the CRASH 2 trial. It was a massive (20,211 patients) RCT that demonstrated an all cause mortality benefit of 1.5% with the use of TXA. (CRASH-2 2010) However, despite being a groundbreaking trial, there are some significant, which I discuss further in my main post on the trial. TXA did not decrease the number of people requiring a transfusion, the total amount of blood transfused, nor the number of patients requiring surgery, which raises the question of its mechanism of action. Neurologically intact survival was not statistically significant. I am also cautious in my interpretation of harms from this trial, as many patients were enrolled in remote centers where thromboembolism may be more likely to be missed. The rate of thromboembolism is much higher in a similar American trauma cohort. (Erramouspe 2020) Finally, the results may not extrapolate well to centers with advanced trauma care.
There is another RCT looking at TXA in trauma. The STAAMP trial is a pragmatic, phase 3, multicenter, double-blind, placebo controlled RCT comparing TXA to placebo in the prehospital setting in trauma patients with hypotension or tachycardia. (Guyette 2020) There was no difference in the primary outcome of 30 day mortality (8.1% vs 9.9%, p=0.17). All of their pre-specified subgroup analyses were also statistically negative. They added a couple extra analyses that are reported as positive for TXA, but it is hard to put a lot of faith in these, as adding analyses not in the protocol significantly increases the risk of bias. The point estimates do favour TXA, so this trial may simply be under-powered for a very small beneficial effect from TXA (but that also leaves it very underpowered for harms).
There are a few observational trials that are commonly said to support the use of TXA in trauma, but have some significant limitations because of their observational methodology. The MATTERS trial was a retrospective, single centre trial from a single military hospital in Afghanistan. They looked at 896 patients who received at least 1 unit of packed red blood cells after admission for a traumatic injury. TXA was associated with lower mortality (17.4% vs 23.9%, p=0.03) and the benefit was larger among patients who required massive transfusion (14.4% vs 28.1%). It is strange to me that among patients receiving TXA, the “sicker group” requiring massive transfusion actually had a lower mortality than the overall group (14.4% vs 17.4%). That isn’t biologically plausible, and to me is a strong indication of the fallibility of this data and the possible unseen underlying confounders. Thrombotic complications were higher in the TXA group (5.1% vs 0.5%), which could be an indication of real world risks, or again an indication of confounding. Furthermore, transfusion requirements were higher in the TXA group, which is funny for a drug that is supposed to limit bleeding. That might be an example of survivorship bias, an indication that TXA doesn’t actually stop bleeding, or a hint that perhaps we don’t truly understand TXA’s mechanism of action. (Morrison 2012) The MATTERS trial was extended in MATTERS II – but the cohort overlaps with the one reported in the original publication. (Morrison 2013)
There is also an observational study looking at TXA in a civilian population that is frequently said to support the use of TXA, but I actually think the numbers might say the opposite. (Cole 2015) They include 465 patients over 15 years of age who were admitted to the critical care unit and had an ISS more than 14. (Seeing as we don’t know who will be admitted to critical care, these inclusion criteria are not usable clinically, and introduce significant selection bias.) The groups were unbalanced at the outset, as this isn’t randomized data, so any comparisons are very difficult. In the first 48 hours, morality was the same in both groups (8%), but after 48 hours mortality was actually higher in the TXA group (8% vs 11%). The TXA group received more total blood (7.4 vs 5 units), which could either indicate that they were sicker, or that TXA doesn’t help with bleeding. The finding that is frequently talked about from this trial is that there was lower early mortality in the group of patients with shock (11% vs 15%). However, that finding requires layering multiple different subgroups, and ignores the fact that morality after 48 hours was higher with TXA (11% vs 8%), so that overall mortality was identical even in this subgroup. It is hard to make too much from this data, as confounders could push the results in either direction, but if you are citing this data it is important to note that mortality was actually higher in the TXA group (but they were also probably sicker).
The available data is mostly limited to adult patients, but the PECARN group currently has the TIC-TOC study underway – an RCT looking at TXA in pediatric trauma patients – so we will see more data in the future. (NCT02840097)
Isolated head trauma
There is a lot more debate about the use of TXA for isolated head trauma. The biggest trial – CRASH 3 – was negative, but with a promising subgroup and secondary analyses that has led some to interpret it as positive. (CRASH 3 2019) (The problems with subgroups are discussed more below.) A full write up on CRASH-3 can be found here, but the quick summary is that this is a massive RCT of more than 12,000 patients with isolated traumatic brain injury which demonstrated no change in mortality and no change in neurologic outcomes.
There is also a prehospital RCT looking at TXA for traumatic brain injury which enrolled 966 patients. (Rowell 2020) The details are here, but again this trial found no difference in mortality or neurologic outcomes. The big problem with this study is that many of the patients actually had very mild injuries, which isn’t always obvious in the prehospital setting.
A meta-analysis of the trials looking at TXA for traumatic brain injury concludes “in patients with acute TBI, TXA probably has no effect on mortality or disability.” (Lawati 2020)
CRASH 2 FOAMed: First10EM, EMCrit, SGEM, St. Emlyn’s, Maryland CC
CRASH 3 FOAMed: First10EM, REBEL EM, SGEM, PulmCrit, EMNerd, St Emlyn’s
MATTERS FOAMed: Short Coat
TXA Timing
Although it is widely preached that TXA must be given early, the data supporting this claim is pretty weak. (Of course, much like with antibiotics for sepsis, if you know you are going to give a drug, there is no reason to delay.)
The contention that earlier is better is based on a subgroup in CRASH-2. Patients treated in less than 3 hours had decreased mortality, but those treated in more than 3 hours had increased mortality. Of course, subgroups are frequently misleading (see below), and this association has numerous potential confounders. Why were patients treated later? What was different about their care?
There is a meta-analysis in the WOMAN trial that appears to confirm this association, but is actually a travesty of science that I am surprised made it past the editors. The researchers combined all cause mortality from CRASH-2 with disease specific mortality from WOMAN, making the results completely meaningless.
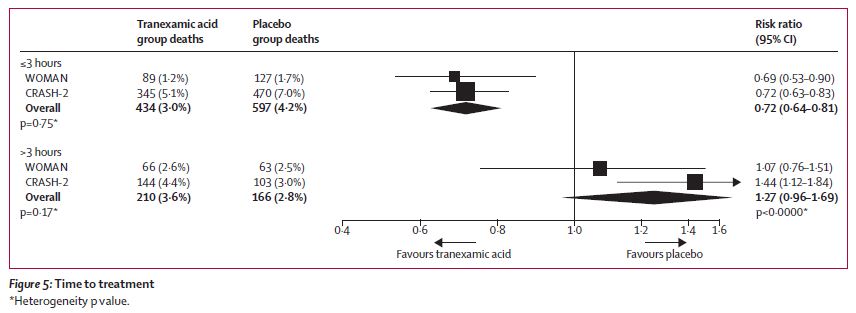
Conversely, there doesn’t seem to be any effect of time to treatment in HALT-IT, TICH-2, or CRASH-3. Overall, I think the science supporting a time dependent effect for TXA is very weak, and I am not sure that we should be making clinical decisions based on this association.
However, if you believe that giving TXA earlier is better, then you also have to accept that giving TXA after 3 hours increases mortality. You can’t accept this subgroup and simultaneously make the claim – which most people do – that TXA is perfectly safe.
Safety
We have huge trials, and I agree with the general sentiment that TXA is relatively safe. However, every medication with biologic effects also has side effects.
The most important safety concern for TXA would be increased mortality. Again, in CRASH-2, TXA increased mortality in the subgroup of patients treated after 3 hours (4.4% vs. 3.1%; RR, 1.44; 95% CI, 1.12Y1.84; p = 0.004). (Napolitano 2013) If the discussion around these papers has taught us anything, it is that people love searching out subgroups and secondary analyses that are positive, but we have a habit of ignoring those that are negative.
This also applies to the ridiculous practice of focusing on disease specific mortality in these massive trials. In the WOMAN trial, all cause mortality was unchanged, but all anyone talks about is death due to bleeding. Similarly, in CRASH-3, all cause mortality was unchanged but “head injury related” death may have been better. However, a decrease in disease specific mortality with no change in all cause mortality just means death from other causes is increased. (In CRASH-3, TXA increased mortality from all other causes with a relative risk of 1.31, 95% CI 0.93-1.85).
Therefore, based on both the time to treatment subgroups and the disease specific mortality secondary analyses, there is an indication that TXA can increase mortality. I don’t actually think that it does, but that is only because I reject the value of the disease specific mortality and time to treatment analyses. If you accept those analyses, then you must accept that you are prescribing a medication that has the potential to kill.
We also have to be very careful about disease oriented outcomes. Many of these trials suggest a decrease in perioperative blood loss, but without an improvement in patient oriented outcomes, this finding can mislead us. Aprotinin is a anti-fibrinolytic similar to TXA that actually seems to reduce perioperative bleeding much more effectively than TXA. (Henry 2011) However, although there were no obvious adverse events in RCTs, it was ultimately pulled from the market because of observational data suggesting cardiovascular complications and an increased mortality. (Henry 2011)
There are some other side effects of TXA to be aware of. There are reports of reports of hypotension after rapid infusion, strokes, and 1 report or TEN. Although the exact mechanism is unclear, TXA has also been associated with seizures, especially post-operatively. (Murkin 2010; Lecker 2016)
It is not really a side effect, but it is interesting to know (and fitting with the physiology of TXA) that it has been implicated in falsely low DDimer levels, resulting in missed PE (which could be important when interpreting the harms in these trials). (Salam 2013)
The big question when it comes to TXA is the risk of thromboembolic disease. The risk was doubled in the HALT-IT trial, but the other RCTs have not found a difference. The observational data is somewhat more concerning, with a 10 fold increase in VTE in the MATTERS trial. (Morrison 2012) This is purely correlational, but I am not sure what confounder would tie TXA use and clots, aside from maybe survivorship bias. Of course, how many PEs one finds is directly related to how hard one looks. I didn’t trust the finding from CRASH-2, when many of the patients were enrolled in centers that didn’t even have a fax machine for randomization. In this setting, missed complications seem likely. However, subsequent trials have looked for VTE more systematically without finding an increase. (Although the interaction between TXA and DDimer could be causing missed diagnoses.) I think TXA likely increase thromboembolic complications, but that the risk is very small and would certainly not be a contra-indication if TXA is actually improving mortality. However, the risk probably needs to be considered when there is no benefit, or when the benefit is only seen in subgroups or disease oriented outcomes. For example, WOMAN demonstrated no change in all cause mortality, and therefore the risk of thromboembolism, although probably tiny, is enough for me to avoid TXA because there is no clear benefit from treating.
A quick note on subgroups
Subgroups and secondary analyses are hypothesis generating only. We repeat this phrase almost as often as we ignore it in medicine. Rather than just parroting the phrase, it is important to understand why EBM folks tell us this. The simple explanation is that repeating tests drastically increases the risk of random findings. It is incredibly unlikely that you will win the lottery after buying a single ticket, but buy enough tickets and you are almost guaranteed to win (somebody wins almost every week).
This is especially important because medicine uses an incredibly low threshold to define “statistically significant”. The p<0.05 is very weak statistical evidence that we should reject the null hypothesis. Many have argued that we should be using much stricter p value cut-offs, or abandoning the p value altogether. (Nakagawa, 2004; Gaudart et al., 2014; Academy of Medical Sciences, 2015) In other areas of science, such as physics, a p value less than 0.0000003 is required before a finding is considered statistically significant. (Johnson, 2014) Thus, even our primary outcomes are prone to being false positive, or positive by chance alone. Adding multiple additional subgroups of secondary analyses significantly increases the risk of false positive findings, which is why we need to be very skeptical of any outcome other than the primary outcome.
How unreliable are subgroups? One study looked at 64 RCTs that made a total of 117 subgroup claims, 46 of which were statistically significant. (Wallach 2017) Only 10% of these were studied in follow-up, and not a single one was corroborated in future research. It is likely that more than 0% of subgroups are true, but using a p value of 0.05, and considering that most of our clinical trials are negative, it probably isn’t much more. Hence, subgroups and secondary analyses are hypothesis generating only.
Mechanism of action?
One of the most confusing aspects to these trials is the purported mechanism of action of TXA. The surgical literature suggested a decrease in blood loss, but without any clinically important changes. Conversely, in CRASH-2 we saw a very important clinical outcome (mortality) but there was no change in the number of people requiring transfusions or total transfusion given. If TXA didn’t actually reduce objective measures of bleeding, how exactly did it prevent death due to bleeding? The same thing happened in the WOMAN trial: the total estimated blood loss, need for transfusions, and total amount transfused were the same in both groups, and yet they claim that TXA reduced “death due to bleeding”. (Given that all cause mortality wasn’t changed, this is a strong indication that the “death due to bleeding” is just statistical nonsense or misclassification.)
Importance of replication
Replication is the bedrock of science. The attempt to replicate studies and falsify prior results is the core of the scientific method, and the only route to certainty.
Inherently, I think we all understand the reason for this. Flukes happen. If your friend throws a dart and it hits the bullseye, you don’t let them claim that they are the greatest darts player of all time based on that one throw. You ask them to do it again. Replication reduces the risk that what you are seeing was a fluke.
The more you do something, the more common individual flukes will be. If you throw a million darts, one is likely to hit the bullseye. That is a problem for research, because every year there are literally millions of publications added to PubMed. Flukes will happen. We need to verify positive studies.
Even more important than mathematical flukes is bias. Even great trials will have some sources of bias – things that push the trial results away from the truth.
Thus, for every positive trial, there are three possibilities: it could be a mathematical fluke, it could be positive because of bias, or it could be a true finding. The only way to sort these options out is replication.
When it comes to TXA, CRASH-2 is a massive trial, which makes a mathematical fluke pretty unlikely (but not impossible). It was a great trial, but it wasn’t perfect (no trial is), so the results could be from bias. It is clearly a good enough study that we should be prescribing TXA to our trauma patients, but its size and its quality don’t negate the need for replication, because replication is the core of the scientific process.
Summary
Taken together, I think these studies make it clear that TXA is not a miracle cure. It might have a small physiologic effect, but there are more negative trials than there are positive. With the sole exception of CRASH-2, the high quality studies are all negative. The rest of the benefit is seen in disease oriented outcomes in small, low quality studies. That really makes me wonder whether CRASH-2 represents a false positive, outlying result. The only way to know would be a repeat study, which seems unlikely, but – although we tend to ignore the fact in medicine – replication is the foundation of science.
My personal feeling, informed by the totality of the TXA literature, is that a CRASH-2 replication has a high probability of being negative – that there is still equipoise. If such a study were done in a country with an advanced trauma system, it is even more likely to be negative. However, the best available evidence at this point supports TXA in bleeding trauma patients.
Clinically speaking, I use TXA in bleeding trauma patients. I don’t use it in isolated traumatic brain injury. I don’t use it in spontaneous intracranial hemorrhage or subarachnoid hemorrhage. I don’t use it in postpartum hemorrhage. I don’t use it for gastrointestinal bleeding. I have been using it in epistaxis, but should probably stop.
For most other indications, the science is too uncertain to make strong conclusions. In totality, TXA seems to have a very small effect (if any). It probably shouldn’t be used routinely for any indication. Harms are probably small, and probably even smaller when used topically, but shouldn’t be overlooked. For select patients with bleeding issues, especially those uncontrolled by other means, it may still be reasonable to try TXA while waiting for more research to be done.
Other FOAMed
Tranexamic Acid (TXA), Crash 2, & Pragmatism with Tim Coats – EMCrit
Tranexamic Acid (TXA) for Everything that Bleeds? – REBEL EM
References
Academy of Medical Sciences (2015) Academy of Medical Sciences Reproducibility and reliability of biomedical research: improving research practice. Academy of Medical Sciences, BBSRC, MRC, Wellcome Trust Symposium report. 2015
Armellin G, Casella S, Guzzinati S, Pasini L, Marcassa A, Giron G. Tranexamic acid in aortic valve replacement. Journal of cardiothoracic and vascular anesthesia. 2001; 15(3):331-5. [pubmed]
Atabaki P, Samarei R, Aribi MS, Soheili A, Mehryar HR. A comparative study on the effect of topical phenylephrine with topical tranexamic acid in management of epistaxis. Journal of the Urmia Nursing and Midwifery Faculty 2017; 15(7):488–96.
Ayedi M, Jarraya A, Smaoui M, Zouari J, Smaoui L, Kolsi K. Effect of tranexamic acid on post partum hemorrhage by uterine atony: A preliminary result of a randomized, placebocontrolled trial. European Journal of Anaesthesiology. 2011;28:165.
Baharoglu MI, Germans MR, Rinkel GJ, et al. Antifibrinolytic therapy for aneurysmal subarachnoid haemorrhage. The Cochrane database of systematic reviews. 2013; PMID: 23990381
Barer D, Ogilvie A, Henry D, et al. Cimetidine and tranexamic acid in the treatment of acute upper-gastrointestinal-tract bleeding. The New England journal of medicine. 1983; 308(26):1571-5. [pubmed]
Bennett C, Klingenberg SL, Langholz E, Gluud LL. Tranexamic acid for upper gastrointestinal bleeding. The Cochrane database of systematic reviews. 2014; [pubmed]
Bryant-Smith AC, Lethaby A, Farquhar C, Hickey M. Antifibrinolytics for heavy menstrual bleeding . 2018;
Chan CC, Chan YY, Tanweer F. Systematic review and meta-analysis of the use of tranexamic acid in tonsillectomy. European archives of oto-rhino-laryngology. 2013; 270(2):735-48. [pubmed]
Cole E, Davenport R, Willett K, Brohi K. Tranexamic acid use in severely injured civilian patients and the effects on outcomes: a prospective cohort study. Annals of surgery. 2015; 261(2):390-4. [pubmed]
CRASH-2 trial collaborators, Shakur H, Roberts I, et al. Effects of tranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients with significant haemorrhage (CRASH-2): a randomised, placebo-controlled trial. Lancet (London, England). 2010; 376(9734):23-32. PMID: 20554319
CRASH 3 Trial Collaborators. Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH 3): a randomised, placebo-controlled trial. Lancet (London, England). 2019; PMID: 31623894
Daneshmend TK, Hawkey CJ, Langman MJ, Logan RF, Long RG, Walt RP. Omeprazole versus placebo for acute upper gastrointestinal bleeding: randomised double blind controlled trial. BMJ. 1992;304:(6820)143-7. [pubmed]
Ducloy-Bouthors AS, Jude B, Duhamel A, et al. High-dose tranexamic acid reduces blood loss in postpartum haemorrhage. Critical care (London, England). 2011; 15(2):R117. [pubmed]
Erramouspe PJ, García-Pintos MF, Benipal S, Manoukian MAC, Santamarina JL, Shawagga HG, Vo LL, Galante JM, Nishijima D. Mortality and Complication Rates in Adult Trauma Patients Receiving Tranexamic Acid: A Single-center Experience in the Post-CRASH-2 Era. Acad Emerg Med. 2020 May;27(5):358-365. PMID: 32189440
Gaudart J, Huiart L, Milligan PJ, Thiebaut R, Giorgi R. Reproducibility issues in science, is P value really the only answer? Proc Natl Acad Sci U S A. 2014 May 13;111(19):E1934. doi: 10.1073/pnas.1323051111. Epub 2014 Apr 23. PMID: 24760820; PMCID: PMC4024892.
Gharaibeh A, Savage HI, Scherer RW, Goldberg MF, Lindsley K. Medical interventions for traumatic hyphema. The Cochrane database of systematic reviews. 2019; 1:CD005431. [pubmed]
Guyette FX, Brown JB, Zenati MS, et al. Tranexamic Acid During Prehospital Transport in Patients at Risk for Hemorrhage After Injury: A Double-blind, Placebo-Controlled, Randomized Clinical Trial. JAMA Surg. 2020 Oct 5;156(1):11–20. PMID: 33016996
Henry DA, Carless PA, Moxey AJ, O’Connell D, Stokes BJ, Fergusson DA, Ker K. Anti-fibrinolytic use for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev. 2011 Jan 19;(1):CD001886. doi: 10.1002/14651858.CD001886.pub3. Update in: Cochrane Database Syst Rev. 2011;(3):CD001886. PMID: 21249650
Hunt BJ. The current place of tranexamic acid in the management of bleeding. Anaesthesia. 2015 Jan;70 Suppl 1:50-3, e18. doi: 10.1111/anae.12910. PMID: 25440395
Johnson VE. Reply to Gelman, Gaudart, Pericchi: More reasons to revise standards for statistical evidence. Proc Natl Acad Sci U S A. 2014 May 13;111(19):E1936-7. doi: 10.1073/pnas.1400338111. PMID: 24940581; PMCID: PMC4024871.
Joseph J, Martinez-Devesa P, Bellorini J, Burton MJ. Tranexamic acid for patients with nasal haemorrhage (epistaxis). The Cochrane database of systematic reviews. 2018; 12:CD004328. [pubmed]
Karadaş A, Doğan NÖ, Pinar SG, et al. A randomized controlled trial of the effects of local tranexamic acid on mortality, rebleeding, and recurrent endoscopy need in patients with upper gastrointestinal hemorrhage. European journal of gastroenterology & hepatology. 2020; 32(1):26-31. [pubmed]
Lawati, K.A., Sharif, S., Maqbali, S.A. et al. Efficacy and safety of tranexamic acid in acute traumatic brain injury: a systematic review and meta-analysis of randomized-controlled trials. Intensive Care Med (2020). https://doi.org/10.1007/s00134-020-06279-w
Lecker I, Wang DS, Whissell PD, Avramescu S, Mazer CD, Orser BA. Tranexamic acid-associated seizures: Causes and treatment. Annals of neurology. 2016; 79(1):18-26. [pubmed]
Madden A, Hulme P. BET 2: Topical tranexamic acid in postcircumcision bleeding Emerg Med J. 2021; 38(4):322.3-323.
Morrison JJ, Dubose JJ, Rasmussen TE, Midwinter MJ. Military Application of Tranexamic Acid in Trauma Emergency Resuscitation (MATTERs) Study. Archives of surgery (Chicago, Ill. : 1960). 2012; 147(2):113-9. [pubmed]
Morrison JJ, Ross JD, Dubose JJ, Jansen JO, Midwinter MJ, Rasmussen TE. Association of cryoprecipitate and tranexamic acid with improved survival following wartime injury: findings from the MATTERs II Study. JAMA surgery. 2013; 148(3):218-25. [pubmed]
Murkin JM, Falter F, Granton J, Young B, Burt C, Chu M. High-dose tranexamic Acid is associated with nonischemic clinical seizures in cardiac surgical patients. Anesth Analg. 2010 Feb 1;110(2):350-3. PMID: 19996135
Myles PS, Smith JA, Forbes A, et al. Tranexamic Acid in Patients Undergoing Coronary-Artery Surgery N Engl J Med. 2017; 376(2):136-148.
Nakagawa S. A farewell to Bonferroni: the problems of low statistical power and publication bias . 2004; 15(6):1044-1045.
Napolitano LM, Cohen MJ, Cotton BA, et al. Tranexamic acid in trauma: how should we use it? J Trauma Acute Care Surg 2013; 74: 1575-1586.
Petruson B. A double blind study to evaluate the effect on epistaxis with oral administration of the antifibrinolytic drug tranexamic acid (Cyklokapron®). Acta Otolaryngologica 1974;77(Suppl 317):57‐61.
Perel P, Ker K, Morales Uribe CH, Roberts I. Tranexamic acid for reducing mortality in emergency and urgent surgery. Cochrane Database Syst Rev. 2013;1:CD010245.
Prutsky G, Domecq JP, Salazar CA, Accinelli R. Antifibrinolytic therapy to reduce haemoptysis from any cause . Cochrane Database of Systematic Reviews 2016, Issue 11. Art. No.: CD008711.
Reuben A, Appelboam A, et al. The use of tranexamic acid to reduce the need for Nasal Packing in Epistaxis (NoPac): randomised controlled trial. Annals of Emergency Medicine. 2021. 10.1016/j.annemergmed.2020.12.013
Roberts I., Coats T., Edwards P., Gilmore I., Jairath V., Ker K., Manno D., Shakur H., Stanworth S., Veitch A. (2014). HALT-IT–tranexamic acid for the treatment of gastrointestinal bleeding: study protocol for a randomised controlled trial. Trials, Nov 19;15:450.
Rowell SE, Meier EN, McKnight B, et al. Effect of Out-of-Hospital Tranexamic Acid vs Placebo on 6-Month Functional Neurologic Outcomes in Patients With Moderate or Severe Traumatic Brain Injury. JAMA. 2020 Sep 8;324(10):961-974. doi: 10.1001/jama.2020.8958. PMID: 32897344
Ruiz W. (thesis) [Acido tranexamico vs placebo en hemoptisis por TBC pulmonar: estudio pilato doble ciego]. 1994.
Sahhaf F, Abbasalizadeh S, Ghojazadeh M, Velayati A, Khandanloo R, Saleh P, Piri R, Naghavi-Behzad M. Comparison effect of intravenous tranexamic acid and misoprostol for postpartum haemorrhage. Niger Med J 2014;55:348-53
Salam A, King C, Orhan O, Mak V. The great deception: tranexamic acid and extensive pulmonary emboli Case Reports. 2013;
Sentilhes L, Winer N, Azria E, et al. Tranexamic Acid for the Prevention of Blood Loss after Vaginal Delivery. The New England journal of medicine. 2018; 379(8):731-742. [pubmed]
Sprigg N, Flaherty K, Appleton JP, et al. Tranexamic acid for hyperacute primary IntraCerebral Haemorrhage (TICH-2): an international randomised, placebo-controlled, phase 3 superiority trial. Lancet (London, England). 2018; 391(10135):2107-2115. PMID: 29778325 [free full text]
Tscheikuna J, Chvaychoo B, Naruman C, Maranetra N. Tranexamic acid in patients with hemoptysis. Journal of the Medical Association of Thailand = Chotmaihet thangphaet. 2002; 85(4):399-404. [pubmed]
Wallach JD, Sullivan PG, Trepanowski JF, Sainani KL, Steyerberg EW, Ioannidis JPA. Evaluation of Evidence of Statistical Support and Corroboration of Subgroup Claims in Randomized Clinical Trials JAMA Intern Med. 2017; 177(4):554-.
Wand O, Guber E, Guber A, Epstein Shochet G, Israeli-Shani L, Shitrit D. Inhaled Tranexamic Acid TXA for Hemoptysis Treatment: A Randomized Controlled Trial. Chest. 2018; 154(6):1379-1384. PMID: 30321510
White A, O’Reilly BF. Oral tranexamic acid in the management of epistaxis. Clinical otolaryngology and allied sciences. 1988; 13(1):11-6. [pubmed]
WOMAN trial collaborators . Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial. Lancet (London, England). 2017; PMID: 28456509 [free full text]
Zahed R et al. 2013. A new and rapid method for epistaxis treatment using injectable form of tranexamic acid topically: a randomized controlled trial. Am J Emerg Med. 31(9):1389-92. PMID: 23911102
Morgenstern, J. Does TXA work for everything? For anything?, First10EM, June 28, 2021. Available at:
https://doi.org/10.51684/FIRS.79621
4 thoughts on “Does TXA work for everything? For anything?”
Two important things I wanted to highlight that are especially great about this amazing write up :
1) The thing about aprotinin and that it on paper seems more effective but still does worse in a trial , is a notion Jerome Hoffman talks about in this lecture . The argument being that we make drugs that are too good to do a specific thing in the body , and we may find out that we are not that informed about the complex physiology as we might have thought. Hoffman talks about warfarin being the worst drug in the world but is still around because it strikes a balance in the body that “more effective drugs” that are more specifically targeted don’t manage . TXA may be a new warfarin https://m.youtube.com/watch?v=49Q0bp_BZZU (13:00-15:00)
2) Also an important point about subgroup analysis , that you highlight and I’ve heard Hoffman highlight before: When you begin doing subgroup analysis it’s a finite system / enclosed system . So when you see benefit in one subgroup ( I.e TXA <3h in trauma) then you must also logically buy the argument that the other subgroup in this post-hoc finite system is harmful (if one group “goes up” the other must “come down”).
Or just don’t believe the argument posed by post-hoc analysis before further studied .
Very well explained , Justin – thanks !!