
N95 masks are designed to be single use. In normal times, they shouldn’t be reworn. In normal times, they shouldn’t be decontaminated and reused. But these are not normal times. COVID-19 has resulted in drastic PPE shortages around the world, and has left many hospital systems considering options for reusing their normally disposable equipment. This is a controlled study looking at 4 different possible techniques for decontaminating and reusing N95 masks.
The paper
Fischer RJ, Morris DH, van Doremalen N, et al. Assessment of N95 respirator decontamination and re-use for SARS-CoV-2. 2020. Prepublished online.
The Methods
This is a laboratory based study, in which 4 different N95 decontamination methods were compared. The 4 methods were UV radiation, 70 degree Celsius heat, 70% ethanol, and vaporized hydrogen peroxide. (If you are actually using these methods, it is probably worth reading the paper to delve into the details.) They looked at each method’s ability to reduce contamination of SARS-CoV-2, and they also assessed the effect of each method on respirator function.
Decontamination was measured by performing titrated viral cultures at various time frames after each decontamination method and on a control.
Respirator function was determined by quantitative testing, using the “Portacount Respirator fit tester”, which measures aerosols both inside and outside the mask. They did dynamic testing, in that they had participants move and talk while wearing the mask. The results are reported as the “fit factor”, which is the ratio of particles outside the mask to those inside. (A fit factor of 100 is considered a requirement for the mask to pass this test.)
The Results
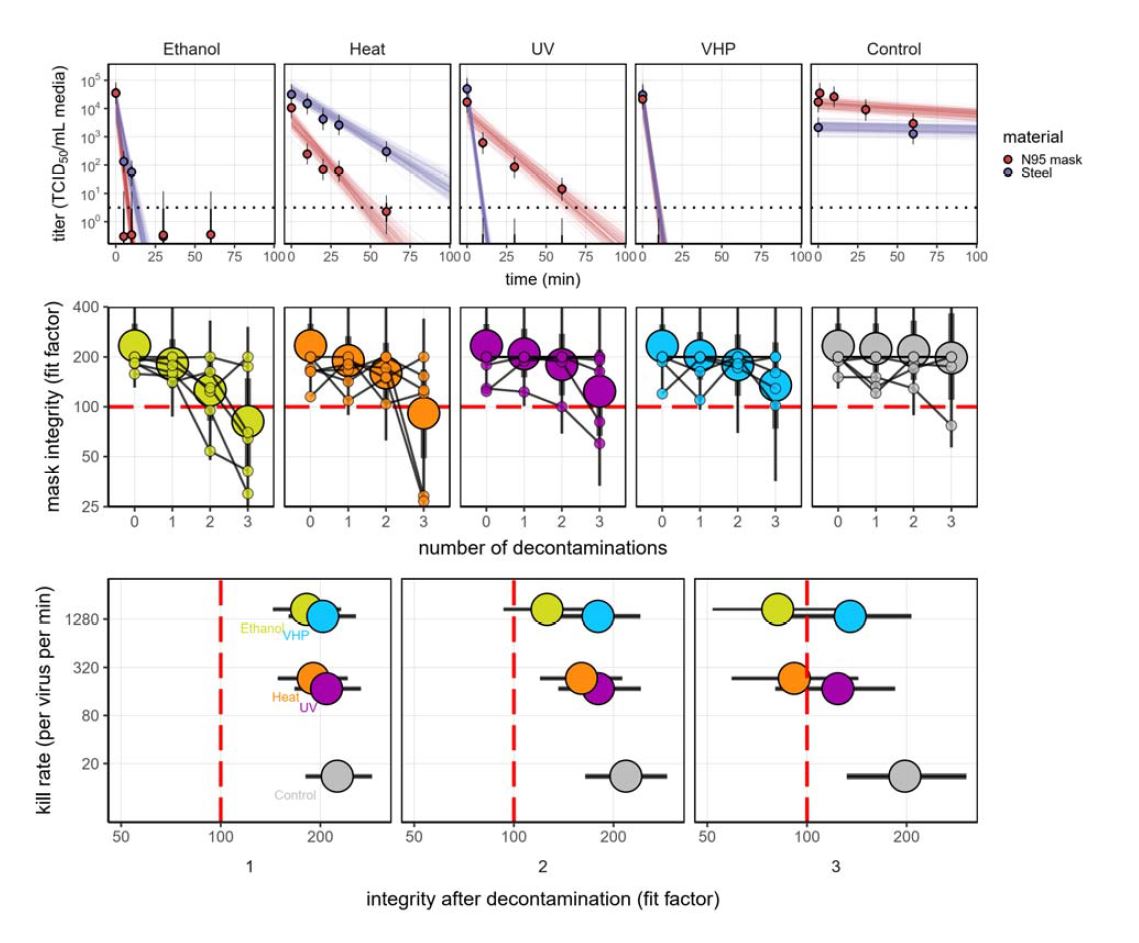
The only technique that completely eliminated the virus was the vaporized hydrogen peroxide, but they only performed cultures up to 100 minutes. Given enough time, UV light and heat both look like they might also have eliminated all the virus, but that wasn’t actually demonstrated, and longer times might have significant impacts on the integrity of the masks. The ethanol technique is not time based, but rather based on the number of applications. 5 applications of 70% ethanol DOES NOT completely eliminate the virus, which the authors say is consistent with prior research.
The median time until only 1 in 1 million viral particles remained alive was:
- Control: 1550 minutes
- Ethanol: 13 minutes
- Heat: 93 minutes
- UV: 125 minutes
- Vaporized hydrogen peroxide: 16 minutes
The integrity of all masks decreased with each decontamination. Looking at just the point estimates, integrity was fine for all methods after the first decontamination, but fell below acceptable levels after the second decontamination with ethanol, and the third decontamination with UV light and heat. However, the 95% confidence intervals cross the accepted integrity target after 2 decontamination cycles for every method, so until we have better data, it appears that 1 decontamination cycle should be the max. (The average here is much less important than the worst numbers seen, as we can’t afford to have ineffective masks being reused.)
My thoughts
This is a really valuable study, and reassures me that N95s can be decontaminated and reused, at least a limited number of times. Ideally though, we would want to see a lot more data before adopting such a high risk, novel intervention.
In terms of decontamination, the authors seem really focused on the speed that the virus was killed. I am not sure that speed is the most important outcome. If 100% of the virus is killed, I don’t really care if it takes 10 minutes or 10 hours. Obviously, this matters in terms of the efficiency of the process, but by itself, speed should not be the deciding factor. Assuming a technique can be shown to be 100% effective, we should ignore the speed of the technique, and focus on the longevity and integrity of the masks.
It is hard to tell from their discussion section, but I think they only tested the decontamination on discs cut out of an N95 mask. (They did decontaminate full masks to test their integrity, but I believe the viral cultures were done on small pieces of N95 material rather than full masks.) This is an issue, as discs are likely easier to decontaminate. Masks have complex geometry and are likely to fold. Decontamination methods might not work as well in crevices as they do on flat pieces of fabric.
My big concern is the difference between a proof of concept study that sterilizes a few masks at a time and the industrial processes required to replicate this in bulk. Will the decontamination be less effective with thousands of masks in a machine? Will a large scale operation be more likely to damage masks? How are the masks being transported? When you sterilize 1 mask at a time, they are unlikely to be bent or folded. However, when applying this process to thousands of masks, bending and folding seems much more likely, which could damage the mask, change the fit, or simply block part of the mask from being fully decontaminated. Furthermore, they only tested the integrity of 1 mask (the 3M 9211+), and I could imagine different shaped masks being impacted differently by these techniques.
We also need to be very careful about the extrapolation of these results. They demonstrated that the integrity of the masks might be maintained for 2 or 3 decontaminations, depending on the technique, but there is a clear degradation from all methods. Unfortunately, they didn’t do a fourth decontamination, but the slopes of the curves make it look like the masks would be below the accepted standard after a 4th decontamination in every technique. I am not sure how hospitals are going to track the number of times that masks are decontaminated, but based on this data, there should be a strict limit on that number.
More importantly, we need to interpret this data like we would a non-inferiority or equivalence trial. The point estimate is less important than the 95% confidence interval, because we can’t afford to provide healthcare workers with ineffective masks. The 95% confidence interval crosses the accepted safety standard after 2 decontaminations with every method, so until we have larger data sets, this study tells us that no matter what technique we use, masks should probably not be decontaminated more than once.
Finally, the authors suggest that we should test each of these masks after decontamination before they are used clinically. I think the idea would be that you apply the re-processed mask, and then do one of those qualitative fit tests with the bitter tasting spray. As long as you don’t taste the spray, you know that the mask is safe to use clinically. That certainly makes sense to me, but is a big departure from standard practice, and might require some work to implement.
Bottom line
Based on this laboratory study, vaporized hydrogen peroxide looks like the best option for decontaminating N95 masks while maintaining their integrity. However, this study does not support any more than 1 decontamination, because after that point there is a risk that the integrity of the mask will be substandard.
More COVID-19 posts:
COVID airway management: SAS consensus statement
COVID Resuscitation Principles
COVID Ethics: Should clinicians see patients without appropriate PPE?
Chloroquine for COVID: No good evidence yet
Surviving Sepsis Campaign COVID Guidelines
Antivirals for COVID19 – Not ready for clinical use
Aerosols, Droplets, and Airborne Spread: Everything you could possibly want to know
THE CEBM also has a good post on mask use during COVID
References
Fischer RJ, Morris DH, van Doremalen N, et al. Assessment of N95 respirator decontamination and re-use for SARS-CoV-2. 2020. Prepublished online.
Morgenstern, J. Can we safely reuse N95 masks?, First10EM, April 29, 2020. Available at:
https://doi.org/10.51684/FIRS.19363


12 thoughts on “Can we safely reuse N95 masks?”
Thank you for this one, I am an ER RN in green bay and we are short on n95s so the hospital is trying to give us 2 , and rotate deconing them. Probably far more than they should be after looking at this.
First of all, thank you Justin, for your enlightening publications.
When discussing the health care staff, I find the discussion here to be very valuable.
Yet, I am confused as to the risks for using and reusing N95 and other masks by the general population.
a. At least in my country (Israel), it seems that there is no longer a shortage of masks in the health systems,
b. Here, we are legally bounded to put masks on our faces when going outside.
As I understand it, the chances of getting infected when being exposed to only a few sars-cov-2 viruses is negligible, and only exposure to much higher amount of viruses makes the risk considerable.
Some thoughts by a non-expert (me):
1) A thought: If I’m not mistaken, if we put aside the chances that the general population will not keep other instructions because of false sense of security, then, even a reduction by a factor of 50% in the chances of getting infected is a major thing.
2) A thought: If there are viruses on the inside part of the mask, then we breath them in and out, thus increasing their chances to be settled.
3) A thought: perhaps, the effectiveness of stem, comes partly due to spreading the viruses out of the mask, and only partly by killing them.
4) A wonder: what was the temperature in which the experiment presented here was done? I was surprised that the reduction rate in viruses in the N95 masks was so low in the control group.
Uzi
The use of N95s for healthcare workers is very different from the suggestion for the public to use masks. Healthcare workers use the mask primarily to prevent the virus from getting in. When we suggest the public wear masks, it is primarily to prevent the virus from getting out. (You are probably most symptomatic and shedding the most virus in the 1-2 days before you have any symptoms). For the general public, a surgical mask is more than enough to prevent spreading the virus to the community, and because you are exposed to far less virus, they probably offer adequate protection as well. (I wear a surgical mask or cotton mask when I am out in public, although that happens very rarely right now). We definitely see lots of people wearing masks incorrectly. It needs to stay over the mouth and nose at all times, and if you continuously touch it / readjust it, it definitely could increase your chance of getting infected, as your hands are the most likely place to find virus. However, I still think they should be used. Reuse of the masks worn in public is less of a concern, because unlike the N95 respirators, normal masks don’t require an air-tight fit. (You shouldn’t be wearing an N95 unless you have actually had the fit of the mask tested for your face.)
Thanks for the fast reply.
“You are most symptomatic before you have the symptoms” seems to be a typo or something that I miss?
The instructions here for the general population, is that the mask is for both preventing the virus from getting in and preventing it from going out.
I thought that even though there is non-negligible shedding prior to having symptoms (or when having no clear symptoms) the maximum shedding is when coughs appear.
Also here, most people “use” it incorrectly. Since it is demanded by the law, they put, and I guess that all of them know that it should be put over the mouth and nose, but since it is not so pleasant they put it below the nose, and remove it when they want to speak, at least, if they cough during non-speech, it blocks the spread 🙂
Thanks again.
Correct – that should read “most infectious before you have symptoms”
There is still some debate about this, but I will have a paper out later this week and discuss it on the BroomeDocs podcasts, as well as the St Emlyn’s Journal club, that suggests that 1/2 of all transmission occurs while the patient is asymptomatic.
Excellent post as always.
I agree that a lot more data is needed for fit testing after decontamination. We know these methods work to kill the virus, but I think it is much more concerning that fit may be compromised than if the mask is “dirty.”
This means that fit is far more important to me than if every single viral particle is killed on the outer surface of the mask. This same paper shows much better fit with no decontamination. The half life of the virus means that roughly 1/1000 of the virus is alive after about 12 hours and about 1/1,000,000 of the virus if you go beyond a day. This may still be infectious, but the necessity of a good fit seems to dwarf the risk of a bad fit.
In real world practice, your mask is “dirty” as soon as you see your first patient. You cannot with confidence say that the outer surface of the mask does not have at least some viral particles at any later moment on your shift. We are not (and we should not be) decontaminating our masks mid shift.
I fear we’ve asked the wrong question. We should not ask what kills the virus, but instead what best protects the provider.
Expedited production of N95 masks due to the novel coronavirus pandemic scenario is burgeoning the market growth.
Thank you Justin. It was a hard time…. we have a lab here and also did quite a lot tests on N95. Our result is better not reuse it. But in home, we can try use oven to heat at over 90 degrees 2 minutes. this helps kill virus efficiently.
Since 4 years ago, we try to source reusable masks. I remember in year 2017, I saw one nano fiber masks in an exhibition, Its very impressive, as it can be reused for almost one month. The company is called Suzhou Nice Sweater Clothes Co., Ltd. Their brand is called Nayi. I had one of their mask on their exhibition. Anyone got interest, please try google this company, I can not find their name card now. Hope it hepls.
Why isn’t simple putting a used N-95 mask in a paper bag for seven days examined. There would probably be zero viable viruses remaining and there is NO degradation (no chemical, no heat, no UV). And if someone will argue that there is a remote chance of a viable virus surviving seven days, then my question is this: How many days should the mask be set aside until it may be safely and effectively re-used with ZERO chance of a viable virus remaining. I would LOVE an answer to this question.
This is really lame-brained “research.” You mean it never even occurred to them to examine the anti-viral effectiveness and mask durability of simply hanging a mask up to dry for five days? Sheesh, if “duh” was ever warranted……..
Thanks for sharing this blog. Because coronaviruses lose their viability significantly after 72 hours, many organizations have promoted a rotation and re-use strategy. Assuming there is no soiling and minimal to no viral contamination to the mask, the CDC suggests that masks can be re-used up to 5 times.