There are two handouts that cover the literature surrounding the use of exercise stress testing to risk stratify patients in the emergency department. For part one, I am posting, in its entirety, a critically appraised topic I did as a resident research project during my emergency medicine fellowship year. Part 2 can be found here.
Clinical Question
In emergency department chest pain patients with a normal electrocardiograms and negative cardiac biomarkers, can an exercise stress test predict short term risk for death or myocardial infarct?
Articles Chosen
Amsterdam, E. A., J. D. Kirk, D. B. Diercks, et al. (2002). “Immediate exercise testing to evaluate low-risk patients presenting to the emergency department with chest pain.” Journal of the American College of Cardiology 40(2): 251-6.1
Gomez, M., J. Anderson, L. Karagounis, et al. (1996). “An emergency department-based protocol for rapidly ruling out myocardial ischemia reduces hospital time and expense: results of a randomized study (ROMIO).” Journal of the American College of Cardiology 28(1): 25-33.2
Manini, A. F., A. T. McAfee, V. E. Noble, et al. (2010). “Prognostic value of the Duke treadmill score for emergency department patients with chest pain.” The Journal of Emergency Medicine 39(2): 135-43.3
Meyer, M., R. Mooney and A. Sekera (2006). “A critical pathway for patients with acute chest pain and low risk for short-term adverse cardiac events: role of outpatient stress testing.” Annals of Emergency Medicine 47(5): 435e1-3.4
Scheuermeyer, F., G. Innes, E. Grafstein, et al. (2012). “Safety and Efficiency of a Chest Pain Diagnostic Algorithm With Selective Outpatient Stress Testing for Emergency Department Patients With Potential Ischemic Chest Pain.” Annals of Emergency Medicine.59(4):256.64.5
Bottom Line
Chest pain is a very common complaint in the emergency department, and the estimation of an individual patient’s risk of myocardial infarction is difficult.6 Several guidelines, including those of the American Heart Association and the American College of Cardiology, recommend the use of exercise stress testing to risk stratify patients after negative clinical evaluation, electrocardiogram, and cardiac biomarkers.7-10 In the studies reviewed, exercise stress testing failed to predict myocardial infarctions that occurred in follow-up. There were no deaths in follow-up in these studies. Despite this, all studies concluded that the use of stress testing has a role in the evaluation of chest pain patients with a negative emergency department work-up. The conclusions of these studies highlight the problems with using composite end-points and focusing on the negative predictive value in populations with low baseline risks. Based on this review, there is no evidence to support the routine use of exercise stress testing in low risk chest pain patients.
Search Strategy
Using MEDLINE (1996-Jan. 12, 2012), search (“exercise test” [MeSH] AND “exp chest pain” [MeSH] OR “exp myocardial ischemia” [MeSH] AND “emergency service, hospital” [MeSH] OR “exp emergency medicine” [MeSH]).
Limits: Humans and English language
Yield: 98 results
Titles and abstracts were individually reviewed for content, and 20 articles were identified that evaluated the use of exercise stress testing in the emergency department. Retrospective studies, reviews, and editorials were excluded, leaving 6 prospective trials that evaluated exercise stress testing in the emergency room.
Using Embase (1980-2012 week 2), search (“exercise test” [MeSH] AND “thorax pain” [MeSH] and “exp emergency ward” [MeSH]).
Limits: Humans and English language
Yield: 115 results
Titles and abstracts were individually reviewed for content. Duplicate articles from search #1, retrospective studies, reviews, and editorials were excluded, leaving 3 prospective trials that evaluated exercise stress testing in the emergency room.
These nine articles were reviewed in depth. Two further articles were not included in the final write up because they included such a low risk population (all under the age of 40) that not a single stress test was positive. Finally, two articles, Sanchis 200511 and Sanchis 200612, had to be excluded because the outcomes of interest (death and myocardial infarction) were part of a composite endpoint that included potentially biased and irrelevant endpoints such as revascularization and were never discussed independently. Therefore, this critical appraisal was ultimately limited to 5 relevant studies.
Design
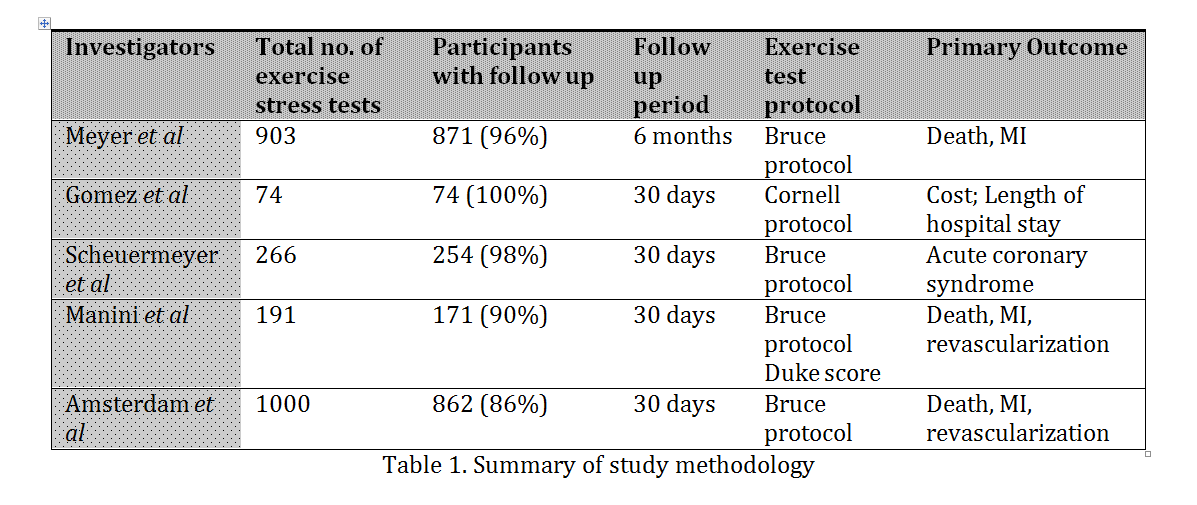
All five studies included a prospective analysis of exercise stress testing and recorded short term death and myocardial infarction as planned primary or secondary outcomes. However, only the Manini study was designed specifically to examine exercise stress testing in emergency department patients already ruled out by ECG and cardiac biomarkers. The studies by Scheuermeyer, Meyer, and Gomez were all designed to examine the impacts of “rapid rule out” protocols for chest pain patients that included exercise stress testing. Finally, Amsterdam and colleagues specifically studied the safety and accuracy of exercise stress testing, but the stress test was done before the results of cardiac biomarkers were known.
Population
The study populations of the selected studies were similar and generally representative of low risk emergency department chest pain patients. The key features that defined patients at low risk were hemodynamic stability, repeated normal electrocardiograms, negative cardiac biomarkers, and a lack of obvious pathology on physical exam, such as congestive heart failure, a new murmur, or an arrhythmia. Two of the studies (Meyer and Gomez) also employed a chest pain risk score, previously validated by Goldman, in the definition of low risk.13 This risk score is highly intuitive and likely representative of standard emergency physician reasoning.
Exclusion criteria were similar in all 5 studies, and included exercise intolerance, difficulty ambulating, paced rhythm, left bundle branch block, and obvious non-cardiac disease such as trauma.
The study by Amsterdam varied significantly from the others, in that patients were not required to have negative cardiac biomarkers prior to exercise stress testing. However, the blood tests were drawn before performing the stress test and results are reported in the paper. Therefore, for the purpose of this critically appraised topic, patients whose first set of biomarkers was reported as positive were excluded from the data analyzed.
Although the study populations were generally similar to Canadian emergency department chest pain patients, the exclusion of patients admitted to hospital with the diagnosis of unstable angina could bias the results. The rate of admission for unstable angina varies significantly between countries and unstable angina is a subjective clinical diagnosis. If patients who would be discharged from a Canadian emergency department were admitted in these studies, the results may be less applicable.
Diagnostic Test
All five studies employed exercise cardiac stress tests. Patients who could not perform the exercise tests were excluded from analysis. Four of the five studies used a standard Bruce protocol and the stated criteria for a positive test were similar. Manini and colleagues employed a standard Bruce protocol, but also collected additional data that allowed them to calculate a Duke score. Gomez and colleagues used the Cornell protocol.
The interpretation of a non-diagnostic exercise stress test varied between the studies. Meyer and Scheuermeyer grouped positive and non-diagnostic tests together as “abnormal”. The other three studies allowed the cardiologist to determine if further testing was warranted in the face of a non-diagnostic exercise stress test. Further work-up was done in 35-100% of patients with non-diagnostic tests. In the specificity and sensitivity calculations presented as part of this appraisal, non-diagnostic tests were grouped with positive tests. This is in keeping with the desire for a test with high sensitivity when looking for the serious outcomes of death or myocardial infarction. Furthermore, analyzing the results in this way represents the highest possible test sensitivity, without altering the calculated specificity.
Outcomes
The primary outcomes of the Amsterdam and Manini studies were death, myocardial infarction, or revascularization. Meyer specifically limited the primary outcome to death and MI, with need for coronary intervention, hospitalization or repeat ED visits being secondary outcomes. Scheuermeyer stated the primary outcome as missed acute coronary syndrome (including unstable angina). The primary outcomes of the Gomez study were cost and length of hospital stay, but the planned secondary outcome was missed diagnoses. Four of the five studies looked at 30 day outcomes, while Meyer looked at outcomes at 6 months.
As stated in the clinical question, the outcomes of interest were limited to those considered to be most clinically important: death and myocardial infarction. In order to be included here, each study had to specifically state the number of deaths and myocardial infarctions. Of note, revascularization and unstable angina were included as composite endpoints with death and MI, and used in the overall conclusions of all the studies.
The importance of revascularization as an outcome for low risk chest pain patients is questionable. With the exception of acute ST elevation myocardial infarction, revascularization does not alter the risk of mortality, nor future myocardial infarction in a population with negative biomarkers.14, 15 Furthermore, angiography and subsequent revascularization will occur as a consequence of a positive stress test but not a negative test, and therefore revascularization is not an independent variable. Revascularization is the result of a clinical decision rather than a disease endpoint. Therefore, it is unclear how predicting the occurrence of revascularization using exercise stress testing benefits emergency department patients.
Similarly, the benefit for emergency department patients of diagnosed unstable angina based on exercise stress testing is unclear. Unstable angina may represent an important clinical outcome, but does not have a clear definition. In these studies, there were no deaths or myocardial infarctions in follow-up in the patients diagnosed with unstable angina. Therefore, the importance of making this diagnosis in the emergency department is questionable. Scheuermeyer included unstable angina in the composite diagnosis of acute coronary syndrome. However, their stated definition of unstable angina included a positive stress test, so this likely represents circular reasoning, with the diagnosis being made on the basis of the test rather than the test being predictive of the diagnosis.
With the exception of the Gomez trial, each study lost patients to follow-up. The number of patients with full follow up data for the Amsterdam, Manini, Meyer, and Scheuermeyer studies was 86%, 90%, 96%, and 98% respectively. Unfortunately, given the very low overall event rate, even a small number of missed deaths or myocardial infarctions could significantly alter the outcomes.
Results
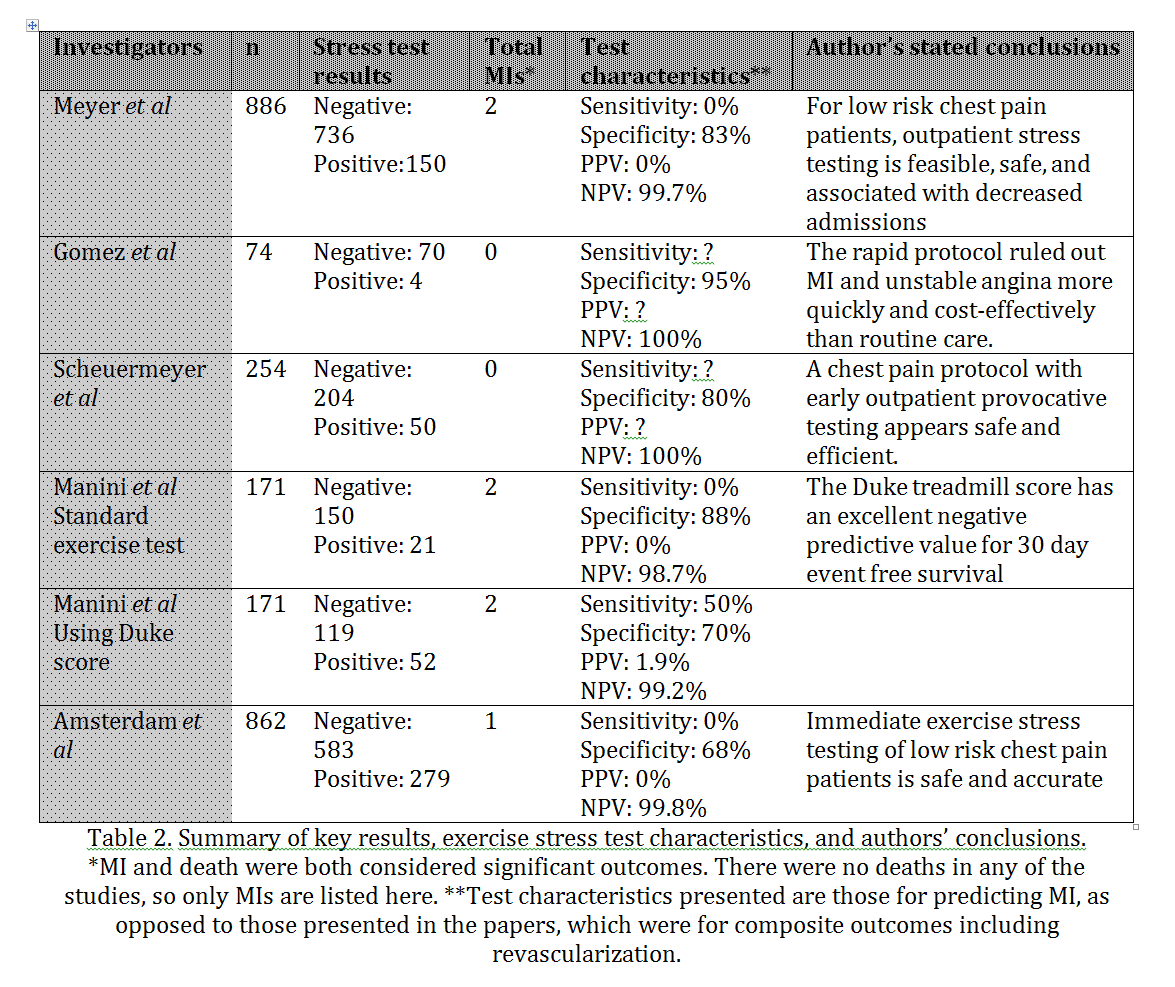
The total number of deaths and myocardial infarctions during the follow up period was very low in all studies. Meyer and colleagues report 0 deaths and 2 myocardial infarctions out of 871 participants. Both MIs were non-ST elevation MIs and occurred in the group with a negative exercise stress test. Gomez and colleagues report 0 deaths and 0 MIs in 74 patients. Scheuermeyer and colleagues also report 0 deaths and 0 MIs on follow up, out of 254 patients with follow up data. Amsterdam and colleagues recorded zero deaths and a single non Q wave MI in an individual with a negative exercise stress test in their study population of 862 patients. In Manini and colleague’s study there were no deaths and two non-ST elevation MIs in 171 patients. Both patients with an MI had negative exercise stress tests by the standard Bruce protocol (however one would have been called high risk using the Duke score).
While the number of events in each study was very small, combined, these studies represent over 2,000 low risk chest pain patients. Using standard criteria, the exercise stress test missed every patient with an important event (all were non-ST elevation MIs) on short term follow-up. The use of the Duke criteria in the Manini study increased the sensitivity of exercise testing for 30 day myocardial infarction incidence from 0% to 50%. However, given the very low absolute risk, the positive predictive value using the Duke criteria was less than 2%.
None of the studies reported adverse events related to exercise stress testing. There were no myocardial infarctions caused by exercise stress testing, and therefore the practice was deemed safe. However, the majority of individuals with positive tests went on to have further invasive testing done, such as nuclear perfusion scans and angiograms, which have their own associated risks. For example, in the Meyer study 150 patients had abnormal exercise stress tests, of whom 32 underwent angiography and 137 underwent a nuclear perfusion scan. Ultimately, 122 of these 150 patients were determined not to have coronary artery disease. In other words, the exercise stress test was ultimately determined to be falsely positive in 81% of patients. If exercise stress testing is neither sensitive nor specific, many patients will be subjected to the risks of further, potentially unnecessary, invasive testing, while still missing patients with short term risk of MI.
Comments
In the assessment of low risk chest pain patients, the emergency physician strives to identify all patients that have, or will develop, an acute coronary syndrome in the weeks following assessment. This ideal is supported by reference to the often incorrectly quoted statistic that mortality is doubled in patients in whom the diagnosis of ACS is missed. (The study, by Pope, that is cited as supporting this fact actually had identical mortality rates in individuals who were initially missed and those who were correctly diagnosed with acute coronary syndrome.)16 Consequently, published guidelines for the management of low risk chest pain patients, such as those disseminated by the American Heart Association and the American College of Cardiology, routinely call for testing beyond clinical assessment, electrocardiograms, and cardiac biomarkers, with exercise stress testing being the test of choice in the absence of contraindications.6-10
There has never been a randomized controlled study to support such a practice.6 Exercise stress testing has limited accuracy in the diagnosis of coronary artery disease, with a sensitivity of 45-68% and a specificity of 77-85% for anatomical disease on angiogram and appears to be even less accurate in women. 6, 17, 18
In the 5 studies presented, standard exercise stress testing missed all myocardial infarctions. The Duke score performed marginally better, but still missed half of the MIs that occurred within 30 days. Pooling all the data, exercise stress testing in these studies has a sensitivity of 0%, a specificity of 78%, a negative predictive value of 99.7%, and a positive predictive value of 0% for the outcome of short term death or myocardial infarction. The problem with focusing on negative predictive value in patients with a low incidence of disease is highlighted by considering that if a physician were to simply send every patient in this cohort home, the negative predictive value of that judgment would have been 99.8% (better than exercise stress testing).
One could argue that even a very small benefit from exercise stress testing would be helpful because the direct risks of exercise stress testing appear to be negligible. However, the subsequent testing that occurs with positive tests must be considered. In these studies (and it seems in general practice), the majority of individuals with a positive exercise stress test went on to have invasive testing such as angiography with or without percutaneous interventions. These procedures have significant risks, such as pericardial tamponade, coronary artery laceration, stroke, allergic reaction to contrast material, and arrhythmias that are reported to occur in about 1 in 1000 procedures.19 It does not make sense to subject patients to this risk when the majority of positive stress tests are false positives. (In the 5 studies, for the outcomes of death and myocardial infarction, 100% of positive stress tests were false positives. For the final diagnosis of coronary artery disease, data is only available from the Meyer study. This study reports an 81% rate of false positive exercise stress tests when using perfusion scans and angiography as gold standards.)
The 5 studies presented do not address other technologies for the assessment of cardiac risk, such as nuclear perfusion scanning or stress echocardiography. However, the results reviewed here emphasize key methodological issues that should be considered when assessing other tests. First, composite outcomes that combine important clinical outcomes such as death and myocardial infarction with surrogate markers such as revascularization can distort results and led to faulty or inappropriate conclusions. Second, the emphasis on a high negative predictive value to support the value of testing is inappropriate in patient populations with a low baseline risk of disease. All tests, even if very inaccurate, will have an impressive negative predictive value when the baseline risk is negligible.
The selected studies demonstrate that in hemodynamically stable chest pain patients without ST changes on ECG and negative cardiac biomarkers, the risk of myocardial infarction in 30 days is low. In the presented papers, there were a total of 5 myocardial infarctions (4 within 30 days and 1 within 6 months) and 0 deaths that occurred in the 2247 patients studied: an event rate of 0.2% or 1/450 patients. This is in keeping with other estimates of a 30 day incidence of death and MI of approximately 1/250 in this population.20 Given this very low baseline risk, further risk stratification by any method would be inherently difficult, if not impossible.6
The low numbers of events in this analysis produce large confidence intervals when assessing the accuracy of exercise stress testing. Additionally, there were a significant number of patients lost to follow up, and even a small number of additional events could significantly alter the results. Thus, a single well designed study of exercise stress testing in low risk emergency department chest pain patients would eclipse these results.
Another potential weakness of this analysis is the focus on short term outcomes. It is possible that the role of exercise stress testing is to identify patients at long term rather than short term risk. First, the follow up period was not a search criterion for this appraisal and no studies of long term outcomes were found. Second, it is not clear how knowledge of long term cardiovascular risk would alter emergency department management of low risk chest pain patients.
In conclusion, it appears that in emergency department chest pain patients with a normal ECG and negative biomarkers, an exercise stress test does not predict the short term risk of death or MI, and potentially exposes a low risk group of patients to the hazards of invasive testing as a consequence of the high incidence of false positive results. Considering the very low risk for “ruled-out” chest pain patients, and the high incidence of false positive results on provocative testing, it could be argued that the emergency physician should not order any further testing in these patients.
Literature Cited
- Amsterdam EA, Kirk JD, Diercks DB, Lewis WR, Turnipseed SD. Immediate exercise testing to evaluate low-risk patients presenting to the emergency department with chest pain. Journal of the American College of Cardiology. 2002;40(2):251-256.
- Gomez M, Anderson J, Karagounis L, Muhlestein J, Mooers F. An emergency department-based protocol for rapidly ruling out myocardial ischemia reduces hospital time and expense: results of a randomized study (ROMIO). Journal of the American College of Cardiology. 1996;28(1):25-33.
- Manini AF, McAfee AT, Noble VE, Bohan JS. Prognostic value of the Duke treadmill score for emergency department patients with chest pain. The Journal of Emergency Medicine. 2010;39(2):135-143.
- Meyer M, Mooney R, Sekera A. A critical pathway for patients with acute chest pain and low risk for short-term adverse cardiac events: role of outpatient stress testing. Annals of Emergency Medicine. 2006;47(5):435e431-433.
- Scheuermeyer F, Innes G, Grafstein E, et al. Safety and Efficiency of a Chest Pain Diagnostic Algorithm With Selective Outpatient Stress Testing for Emergency Department Patients With Potential Ischemic Chest Pain. Annals of Emergency Medicine. 2012;59(4):256-264.
- Kosowsky JM. Approach to the ED patient with “low-risk” chest pain. [Review]. Emergency Medicine Clinics of North America. 2011;29(4):721-727.
- Acute chest pain – evaluation and triage. In: British Columbia Ministry of Health, ed: BCGuidelines.ca; 2008.
- Amsterdam E, Kirk J, Bluemke D, et al. Testing of low-risk patients presenting to the emergency department with chest pain: a scientific statement from the American Heart Association. Circulation. 2010;122(17):1756-1776.
- Gibbons R, Balady G, Beasley J. ACC/AHA guidelines for exercise testing: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Exercise Testing). Circulation. 1997;96(1):345-354.
- Stein RA, Chaitman BR, Balady GJ, et al. Safety and utility of exercise testing in emergency room chest pain centers: An advisory from the Committee on Exercise, Rehabilitation, and Prevention, Council on Clinical Cardiology, American Heart Association. Circulation. 2000;102:1463-1467.
- Sanchis J, Bodi V, Llacer A, et al. Risk stratification of patients with acute chest pain and normal troponin concentrations. Heart. 2005;91(8):1013-1018.
- Sanchis J, Bodi V, Nunez J, et al. Usefulness of early exercise testing and clinical risk score for prognostic evaluation in chest pain units without preexisting evidence of myocardial ischemia. American Journal of Cardiology. 2006;97(5):633-635.
- Goldman L, Cook E, Brand D, et al. A computer protocol to predict myocardial infarction in emergency department patients with chest pain. The New England Journal of Medicine. 1988;318(13):797-803.
- Hoenig M, Aroney C, Scott I. Early invasive versus conservative strategies for unstable angina and non-ST elevation myocardial infarction in the stent era. Chochrane Database Systemic Review. 2010(3:CD004815).
- Stergiopoulos K, Brown D. Initial Coronary Stent Implantation With Medical Therapy vs Medical Therapy Alone for Stable Coronary Artery Disease: Metaanalysis of Randomized Controlled Trials. Archives of Internal Medicine. 2012;172(4):312.
- Pope J, Aufderheide T, Ruthazer R. Missed diagnoses of acute cardiac ischemia in the emergency department. The New England Journal of Medicine. 2000;342(16):1163-1170.
- Amsterdam E, Kirk J, Diercks D, et al. Exercise testing in chest pain units: rational, implentation, and results. Cardiology Clinics. 2005;23:503-516.
- Froelicher V, Lehmann K, Thomas R, et al. The electrocardiographic exercise test in a population with reduced workup bias: diagnostic performance, computerized interpretation, and multivariable prediction. Veterans Affairs Cooperative Study in Health Services #016 (QUEXTA) Study Group. Quantitative Exercise Testing and Angiography. Annals of Internal Medicine. 1998;128(12):965-974.
- Fraker TJ, Fihn S, Gibbons R, Abrams J, Chatterjee K, Daley J. 2007 chronic angina focused update of the ACC/AHA 2002 Guidelines for the management of patients with chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Writing Group to develop the focused update of the 2002 Guidelines for the management of patients with chronic stable angina. Circulation. 2007;116:2762-2772.
- Hollander J, Chang A, Shofer F, McCusker C, Baxt W, Litt H. Coronary computed tomographic angiography for rapid discharge of low-risk patients with potential acute coronary syndromes. Annals of Emergency Medicine. 2009;53(3):295-304.
Morgenstern, J. EBM Lecture Handout #3: Stress testing (part 1), First10EM, June 16, 2015. Available at:
https://doi.org/10.51684/FIRS.514

